Department of Neurosurgery, Queen Elizabeth Hospital Birmingham, Mindelsohn Way, Birmingham, B15 2TH, UK.
Department of Neurosurgery, Royal Hallamshire Hospital, Glossop Road, Sheffield, England, S10 2JF, UK.
Childs Nerv Syst. 2021 Jul;37(7):2177-2186. doi: 10.1007/s00381-021-05165-0. Epub 2021 May 5.
Evidence exists, in CNS germinomas and medulloblastomas (MB), that patient sex significantly influences incidence and outcome. The role of sex genotype in other paediatric CNS tumours remains unclear. This study sought to examine the role of sex genotype in CNS tumour incidence and overall survival (OS).
Age-adjusted incidence and OS rates were collected from the Surveillance Epidemiology and End Result (SEER) registry between 2000 and 2011 for common paediatric (<=19 years) CNS tumours: pilocytic astrocytoma (PA), anaplastic astrocytoma, glioblastoma (GBM), medulloblastoma, supratentorial CNS embryonal tumour, ependymoma, and germinoma. All patients with histologically confirmed, ICD-03 coded, first tumours, were included. Kaplan-Meier and Cox regression analyses were used to calculate hazard ratios (HR).
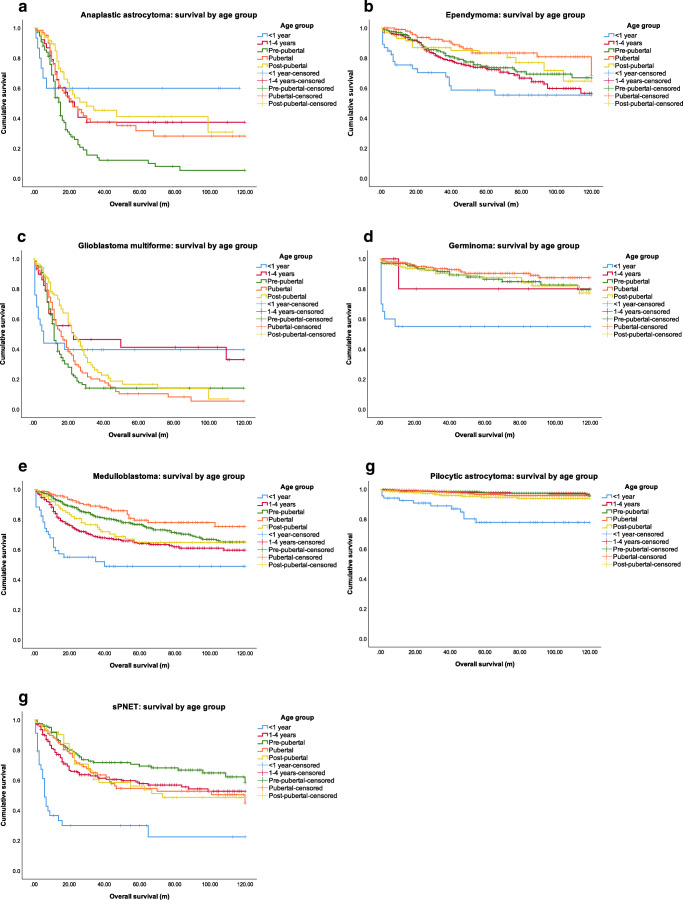
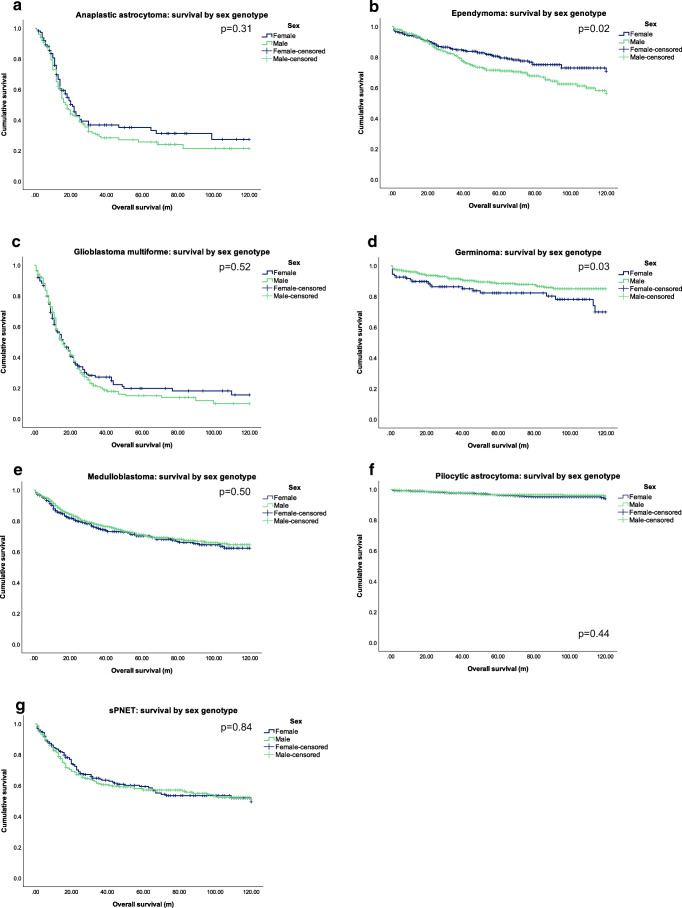
The total cases are as follows: males=3018 and females=2276. Highest incidence was seen in PA (n=2103). GBM displayed the worst OS, whilst PA displayed the best. Higher incidence was observed in males for all tumours, except PA. Females with ependymoma had significantly better OS compared to males, whereas males with germinomas had better OS compared to females. Females <1 year with AA had better OS than males. Increasing age significantly improved male and female survival in ependymoma and medulloblastoma.
Interrogating population-based registries such as SEER minimises bias and provides credible data. Observed differences in incidence and OS between the sexes for different paediatric CNS tumours provide useful prognostic information for clinicians. Sex genotype was a significant independent prognostic factor in ependymomas and germinomas. Further investigation of possible epigenetic and hormonal differences may provide sex-specific vulnerabilities that may be exploitable for targeted therapy.
中枢神经系统生殖细胞瘤和髓母细胞瘤(MB)的证据表明,患者性别显著影响发病率和预后。性基因型在其他小儿中枢神经系统肿瘤中的作用尚不清楚。本研究旨在探讨性基因型在中枢神经系统肿瘤发病率和总生存期(OS)中的作用。
从 2000 年至 2011 年,利用监测、流行病学和最终结果(SEER)登记处收集常见小儿(<=19 岁)中枢神经系统肿瘤的年龄校正发病率和 OS 率:毛细胞星形细胞瘤(PA)、间变性星形细胞瘤、胶质母细胞瘤(GBM)、髓母细胞瘤、幕上中枢神经系统胚胎性肿瘤、室管膜瘤和生殖细胞瘤。所有组织学证实、ICD-03 编码、首次肿瘤的患者均纳入本研究。采用 Kaplan-Meier 和 Cox 回归分析计算风险比(HR)。
总病例数为男性 3018 例,女性 2276 例。PA 发病率最高(n=2103)。GBM 的 OS 最差,而 PA 的 OS 最好。除了 PA,所有肿瘤的男性发病率均较高。与男性相比,女性室管膜瘤的 OS 显著更好,而男性生殖细胞瘤的 OS 则优于女性。AA 女性患者<1 岁的 OS 优于男性。年龄的增加显著改善了男性和女性的生存情况,在室管膜瘤和髓母细胞瘤中尤其如此。
对 SEER 等基于人群的登记处进行调查可以最大程度地减少偏倚并提供可靠的数据。不同小儿中枢神经系统肿瘤性别之间发病率和 OS 的差异为临床医生提供了有用的预后信息。性基因型是室管膜瘤和生殖细胞瘤的独立预后因素。进一步研究可能的表观遗传和激素差异,可能会发现性别特异性的脆弱性,从而为靶向治疗提供依据。