Diagnostic and Research Institute of Pathology, Medical University of Graz, Neue Stiftingtalstrasse 6, 8010, Graz, Austria.
Division of Thoracic Surgery and Hyperbaric Surgery, Department of Surgery, Medical University of Graz, Auenbruggerplatz 29/3, 8036, Graz, Austria.
Sci Rep. 2021 May 7;11(1):9785. doi: 10.1038/s41598-021-89373-3.
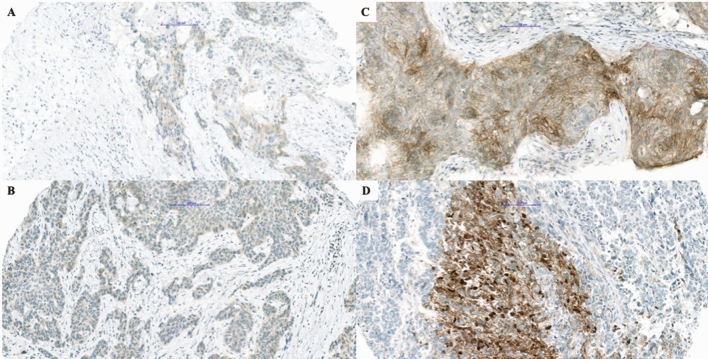
In the last two decades, various therapies have been introduced for lung carcinoma patients, including tyrosine-kinase inhibitors for different mutations. While some of them are specific to specific tumor types, others, like NTRK1-3 fusions, are found in various solid tumors. The occurrence of an NTRK1,2 or 3 fusion acts as a biomarker for efficient treatment with NTRK inhibitors, irrespectively of the tumor type. However, the occurrence of the NTRK1-3 fusions in lung carcinomas is extremely rare. We performed a retrospective analysis to evaluate the applicability of immunohistochemistry with the pan-TRK antibody in the detection of NTRK fusions in lung carcinomas. The study cohort included 176 adenocarcinomas (AC), 161 squamous cell carcinomas (SCC), 31 large-cell neuroendocrine carcinomas (LCNEC), and 19 small cell lung carcinomas (SCLC). Immunohistochemistry (IHC) was performed using the pan-TRK antibody (clone EPR17341, Ventana) on tissue microarrays, while confirmation for all positive cases was done using RNA-based Archer FusionPlex MUG Lung Panel. On IHC staining, 12/387 samples (3.1%) demonstrated a positive reaction. Ten SCC cases (10/161, 6.2%), and two LCNEC cases (2/31, 6.5%) were positive. Positive cases demonstrated heterogeneous staining of tumor cells, mostly membranous with some cytoplasmic and in one case nuclear pattern. RNA-based sequencing did not demonstrate any NTRK1-3 fusion in our patients' collective. Our study demonstrates that pan-TRK expression in lung carcinoma is very low across different histologic types. NTRK1-3 fusions using an RNA-based sequencing approached could not be detected. This stresses the importance of confirmation of immunohistochemistry results by molecular methods.
在过去的二十年中,已经引入了各种针对肺癌患者的治疗方法,包括针对不同突变的酪氨酸激酶抑制剂。虽然其中一些方法针对特定的肿瘤类型,但其他方法,如 NTRK1-3 融合,存在于各种实体瘤中。NTRK1、2 或 3 融合的发生是用 NTRK 抑制剂进行有效治疗的生物标志物,与肿瘤类型无关。然而,肺癌中 NTRK1-3 融合的发生极为罕见。我们进行了一项回顾性分析,以评估使用泛 TRK 抗体进行免疫组织化学检测在肺癌中 NTRK 融合的适用性。研究队列包括 176 例腺癌 (AC)、161 例鳞状细胞癌 (SCC)、31 例大细胞神经内分泌癌 (LCNEC) 和 19 例小细胞肺癌 (SCLC)。使用组织微阵列上的泛 TRK 抗体 (克隆 EPR17341,Ventana) 进行免疫组织化学 (IHC),并使用基于 RNA 的 Archer FusionPlex MUG Lung Panel 对所有阳性病例进行确认。在 IHC 染色中,12/387 个样本 (3.1%) 显示阳性反应。10 例 SCC 病例 (10/161,6.2%) 和 2 例 LCNEC 病例 (2/31,6.5%) 为阳性。阳性病例显示肿瘤细胞的异质性染色,主要为膜性,有些为细胞质性,在 1 例中为核性。基于 RNA 的测序在我们患者的集体中未显示任何 NTRK1-3 融合。我们的研究表明,不同组织学类型的肺癌中泛 TRK 表达非常低。无法通过基于 RNA 的测序方法检测到 NTRK1-3 融合。这强调了通过分子方法确认免疫组织化学结果的重要性。