Department of Medicine and Surgery, University of Insubria, Varese and Department of Medicine and Cardiopulmonary Rehabilitation, Maugeri Care and Research Institute, IRCCS Tradate, Varese, Italy.
Department of Medicine and Surgery, University of Insubria, Varese and Department of Medicine and Cardiopulmonary Rehabilitation, Maugeri Care and Research Institute, IRCCS Tradate, Varese, Italy.
Eur J Intern Med. 2021 Jun;88:1-8. doi: 10.1016/j.ejim.2021.04.019. Epub 2021 Apr 30.
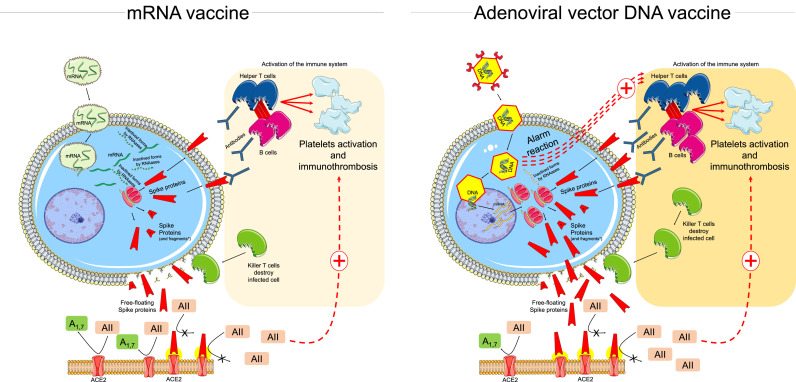
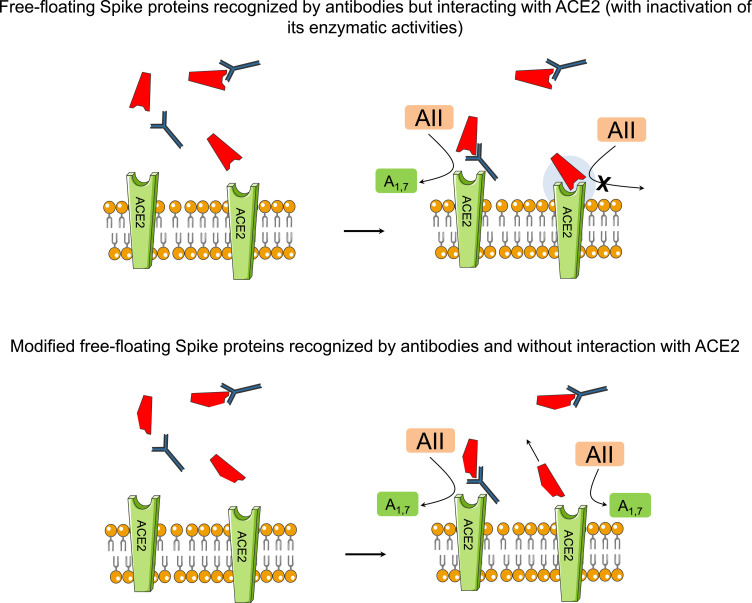
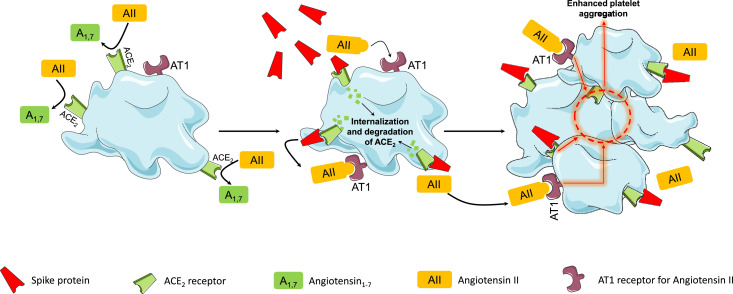
Vaccines to prevent acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection elicit an immune neutralizing response. Some concerns have been raised regarding the safety of SARS-CoV-2 vaccines, largely based on case-reports of serious thromboembolic events after vaccination. Some mechanisms have been suggested which might explain the adverse cardiovascular reactions to SARS-CoV-2 vaccines. Different vaccine platforms are currently available which include live attenuated vaccines, inactivated vaccines, recombinant protein vaccines, vector vaccines, DNA vaccines and RNA vaccines. Vaccines increase the endogenous synthesis of SARS-CoV-2 Spike proteins from a variety of cells. Once synthetized, the Spike proteins assembled in the cytoplasma migrate to the cell surface and protrude with a native-like conformation. These proteins are recognized by the immune system which rapidly develops an immune response. Such response appears to be quite vigorous in the presence of DNA vaccines which encode viral vectors, as well as in subjects who are immunized because of previous exposure to SARS-CoV-2. The resulting pathological features may resemble those of active coronavirus disease. The free-floating Spike proteins synthetized by cells targeted by vaccine and destroyed by the immune response circulate in the blood and systematically interact with angiotensin converting enzyme 2 (ACE2) receptors expressed by a variety of cells including platelets, thereby promoting ACE2 internalization and degradation. These reactions may ultimately lead to platelet aggregation, thrombosis and inflammation mediated by several mechanisms including platelet ACE2 receptors. Whereas Phase III vaccine trials generally excluded participants with previous immunization, vaccination of huge populations in the real life will inevitably include individuals with preexisting immunity. This might lead to excessively enhanced inflammatory and thrombotic reactions in occasional subjects. Further research is urgently needed in this area.
预防严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)感染的疫苗可引发免疫中和反应。由于接种疫苗后出现严重血栓栓塞事件的病例报告,人们对 SARS-CoV-2 疫苗的安全性产生了一些担忧。一些机制被提出,这些机制可能解释了 SARS-CoV-2 疫苗对心血管的不良反应。目前有多种疫苗平台,包括活减毒疫苗、灭活疫苗、重组蛋白疫苗、载体疫苗、DNA 疫苗和 RNA 疫苗。疫苗增加了来自多种细胞的 SARS-CoV-2 刺突蛋白的内源性合成。一旦合成,刺突蛋白在细胞质中组装并以类似天然的构象突出到细胞表面。这些蛋白被免疫系统识别,免疫系统迅速产生免疫反应。在存在编码病毒载体的 DNA 疫苗以及因先前接触 SARS-CoV-2 而免疫的受试者中,这种反应似乎非常强烈。由此产生的病理特征可能类似于活动性冠状病毒病。被疫苗靶向并被免疫反应破坏的细胞合成的游离漂浮的刺突蛋白在血液中循环,并与包括血小板在内的多种细胞表达的血管紧张素转化酶 2(ACE2)受体系统相互作用,从而促进 ACE2 的内化和降解。这些反应可能最终导致血小板聚集、血栓形成和炎症,其机制包括血小板 ACE2 受体。虽然 III 期疫苗试验通常排除了有先前免疫的参与者,但在现实生活中对大量人群进行疫苗接种,不可避免地会包括具有预先存在免疫力的个体。这可能导致偶尔个体中过度增强的炎症和血栓形成反应。在这方面迫切需要进一步的研究。