Huang Yi-Syun, Chiu I-Min, Tsai Ming-Ta, Lin Chun-Fu, Lin Chien-Fu
Department of Emergency Medicine, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan.
Department of Computer Science and Engineering, National Sun Yet-sen University, Kaohsiung, Taiwan.
Front Med (Lausanne). 2021 Apr 22;8:648375. doi: 10.3389/fmed.2021.648375. eCollection 2021.
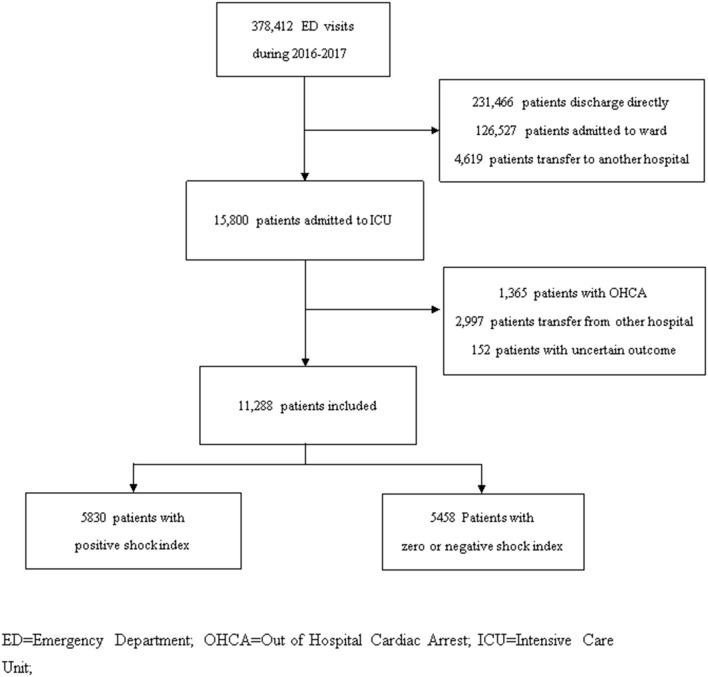
Delta shock index (SI; i.e., change in SI over time) has been shown to predict mortality and need for surgical intervention among trauma patients at the emergency department (ED). However, the usefulness of delta SI for prognosis assessment in non-traumatic critically ill patients at the ED remains unknown. The aim of this study was to analyze the association between delta SI during ED management and in-hospital outcomes in patients admitted to the intensive care unit (ICU). This was a retrospective study conducted in two tertiary medical centers in Taiwan from January 1, 2016, to December 31, 2017. All adult non-traumatic patients who visited the ED and who were subsequently admitted to the ICU were included. We calculated delta SI by subtracting SI at ICU admission from SI at ED triage, and we analyzed its association with in-hospital outcomes. SI was defined as the ratio of heart rate to systolic blood pressure (SBP). The primary outcome was in-hospital mortality, and the secondary outcomes were hospital length of stay (HLOS) and early mortality. Early mortality was defined as mortality within 48 h of ICU admission. During the study period, 11,268 patients met the criteria and were included. Their mean age was 64.5 ± 15.9 years old. Overall, 5,830 (51.6%) patients had positive delta SI. Factors associated with a positive delta SI were multiple comorbidities (51.2% vs. 46.3%, < 0.001) and high Simplified Acute Physiology Score [39 (29-51) vs. 37 (28-47), < 0.001). Patients with positive delta SI were more likely to have tachycardia, hypotension, and higher SI at ICU admission. In the regression analysis, high delta SI was associated with in-hospital mortality [aOR (95% CI): 1.21 (1.03-1.42)] and early mortality [aOR (95% CI): 1.26 (1.07-1.48)], but not for HLOS [difference (95% CI): 0.34 (-0.48 to 1.17)]. In the subgroup analysis, high delta SI had higher odds ratios for both mortality and early mortality in elderly [aOR (95% CI): 1.59 (1.11-2.29)] and septic patients [aOR (95% CI): 1.54 (1.13-2.11)]. It also showed a higher odds ratio for early mortality in patients with triage SBP <100 mmHg [aOR (95% CI): 2.14 (1.21-3.77)] and patients with triage SI ≥ 0.9 [aOR (95% CI): 1.62 (1.01-2.60)]. High delta SI during ED stay is correlated with in-hospital mortality and early mortality in patients admitted to the ICU via ED. Prompt resuscitation should be performed, especially for those with old age, sepsis, triage SBP <100 mmHg, or triage SI ≥ 0.9.
delta休克指数(SI;即SI随时间的变化)已被证明可预测急诊科(ED)创伤患者的死亡率及手术干预需求。然而,delta SI在急诊科非创伤性危重症患者预后评估中的作用尚不清楚。本研究旨在分析急诊科管理期间的delta SI与入住重症监护病房(ICU)患者的院内结局之间的关联。这是一项回顾性研究,于2016年1月1日至2017年12月31日在台湾的两家三级医疗中心进行。纳入所有就诊于急诊科且随后入住ICU的成年非创伤性患者。我们通过用急诊科分诊时的SI减去ICU入院时的SI来计算delta SI,并分析其与院内结局的关联。SI定义为心率与收缩压(SBP)之比。主要结局为院内死亡率,次要结局为住院时间(HLOS)和早期死亡率。早期死亡率定义为ICU入院后48小时内的死亡率。在研究期间,11268例患者符合标准并被纳入。他们的平均年龄为64.5±15.9岁。总体而言,5830例(51.6%)患者的delta SI为阳性。与delta SI为阳性相关的因素有多种合并症(51.2%对46.3%,<0.001)和高简化急性生理学评分[39(29 - 51)对37(28 - 47),<0.001]。delta SI为阳性的患者在ICU入院时更易出现心动过速、低血压和更高的SI。在回归分析中,高delta SI与院内死亡率[aOR(95%CI):1.21(1.03 - 1.42)]和早期死亡率[aOR(95%CI):1.26(1.07 - 1.48)]相关,但与HLOS无关[差值(95%CI):0.34( - 0.48至1.17)]。在亚组分析中,高delta SI在老年患者[aOR(95%CI):1.59(1.11 - 2.29)]和脓毒症患者[aOR(95%CI):1.54(1.13 - 2.11)]中与死亡率和早期死亡率的比值比更高。在分诊SBP<100 mmHg的患者[aOR(95%CI):2.14(1.21 - 3.77)]和分诊SI≥0.9的患者[aOR(95%CI):1.62(1.01 - 2.60)]中,高delta SI与早期死亡率的比值比也更高。急诊科停留期间的高delta SI与经急诊科入住ICU患者的院内死亡率和早期死亡率相关。应迅速进行复苏,尤其是对于老年、脓毒症、分诊SBP<100 mmHg或分诊SI≥0.9的患者。