Wendt Ralph, Thijs Lutgarde, Kalbitz Sven, Mischak Harald, Siwy Justyna, Raad Julia, Metzger Jochen, Neuhaus Barbara, Leyen Heiko von der, Dudoignon Emmanuel, Mebazaa Alexandre, Spasovski Goce, Milenkova Mimoza, Canevska-Talevska Aleksandra, Czerwieńska Beata, Wiecek Andrzej, Peters Björn, Nilsson Åsa, Schwab Matthias, Rothfuss Katja, Lübbert Christoph, Staessen Jan A, Beige Joachim
Department of Infectious Diseases/Tropical Medicine, Nephrology/KfH Renal Unit and Rheumatology, St. Georg Hospital Leipzig, Delitzscher Strasse 141, Leipzig DE 04129, Germany.
Research Unit Hypertension and Cardiovascular Epidemiology, KU Leuven Department of Cardiovascular Diseases, University of Leuven, Belgium.
EClinicalMedicine. 2021 Jun;36:100883. doi: 10.1016/j.eclinm.2021.100883. Epub 2021 May 3.
COVID-19 prediction models based on clinical characteristics, routine biochemistry and imaging, have been developed, but little is known on proteomic markers reflecting the molecular pathophysiology of disease progression.
The multicentre (six European study sites) Prospective Validation of a Proteomic Urine Test for Early and Accurate Prognosis of Critical Course Complications in Patients with SARS-CoV-2 Infection Study (Crit-COV-U) is recruiting consecutive patients (≥ 18 years) with PCR-confirmed SARS-CoV-2 infection. A urinary proteomic biomarker (COV50) developed by capillary-electrophoresis-mass spectrometry (CE-MS) technology, comprising 50 sequenced peptides and identifying the parental proteins, was evaluated in 228 patients (derivation cohort) with replication in 99 patients (validation cohort). Death and progression along the World Health Organization (WHO) Clinical Progression Scale were assessed up to 21 days after the initial PCR test. Statistical methods included logistic regression, receiver operating curve (ROC) analysis and comparison of the area under the curve (AUC).
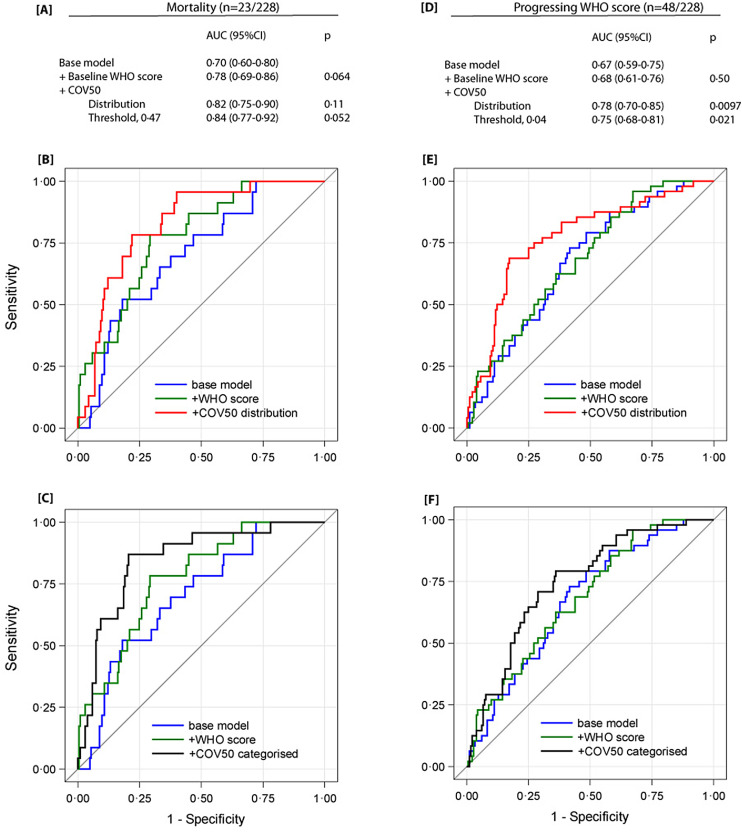
In the derivation cohort, 23 patients died, and 48 developed worse WHO scores. The odds ratios (OR) for death per 1 standard deviation (SD) increment in COV50 were 3·52 (95% CI, 2·02-6·13, <0·0001) unadjusted and 2·73 (1·25-5·95, 0·012) adjusted for sex, age, baseline WHO score, body mass index (BMI) and comorbidities. For WHO scale progression, the corresponding OR were 2·63 (1·80-3·85, 0·0001) and 3·38 (1·85-6·17, 0·0001), respectively. The area under the curve (AUC) for COV50 as a continuously distributed variable was 0·80 (0·72-0·88) for mortality and 0·74 (0·66-0·81) for worsening WHO score. The optimised COV50 thresholds for mortality and worsening WHO score were 0·47 and 0·04 with sensitivity/specificity of 87·0 (74·6%) and 77·1 (63·9%), respectively. On top of covariates, COV50 improved the AUC, albeit borderline for death, from 0·78 to 0·82 ( 0·11) and 0·84 ( 0·052) for mortality and from 0·68 to 0·78 ( 0·0097) and 0·75 ( 0·021) for worsening WHO score. The validation cohort findings were confirmatory.
This first CRIT-COV-U report proves the concept that urinary proteomic profiling generates biomarkers indicating adverse COVID-19 outcomes, even at an early disease stage, including WHO stages 1-3. These findings need to be consolidated in an upcoming final dataset.
The German Federal Ministry of Health funded the study.
基于临床特征、常规生化检查和影像学检查的新型冠状病毒肺炎(COVID-19)预测模型已被开发出来,但对于反映疾病进展分子病理生理学的蛋白质组学标志物却知之甚少。
多中心(六个欧洲研究地点)的新型冠状病毒感染患者重症病程并发症早期准确预后蛋白质组尿检测前瞻性验证研究(Crit-COV-U)正在招募经聚合酶链反应(PCR)确诊的新型冠状病毒感染的连续患者(≥18岁)。采用毛细管电泳-质谱(CE-MS)技术开发的一种尿液蛋白质组学生物标志物(COV50),由50个已测序的肽段组成,并鉴定出其亲本蛋白质,在228例患者(推导队列)中进行了评估,并在99例患者(验证队列)中进行了重复验证。在初次PCR检测后的21天内,评估患者的死亡情况以及按照世界卫生组织(WHO)临床进展量表的进展情况。统计方法包括逻辑回归、受试者工作特征曲线(ROC)分析以及曲线下面积(AUC)比较。
在推导队列中,23例患者死亡,48例患者的WHO评分恶化。COV50每增加1个标准差(SD),未调整的死亡比值比(OR)为3.52(95%CI,2.02-6.13,P<0.0001),在调整性别、年龄、基线WHO评分、体重指数(BMI)和合并症后,OR为2.73(1.25-5.95,P=0.012)。对于WHO量表进展情况,相应的OR分别为2.63(1.80-3.85,P=0.0001)和3.38(1.85-6.17,P=0.0001)。作为连续分布变量的COV50的曲线下面积(AUC),对于死亡率为0.80(0.72-0.88),对于WHO评分恶化情况为0.74(0.66-0.81)。死亡率和WHO评分恶化情况的优化COV50阈值分别为0.47和0.04,敏感性/特异性分别为87.0(74.6%)和77.1(63.9%)。除协变量外,COV50将死亡率的AUC从0.78提高到0.8?(P=0.11)和0.84(P=0.052),将WHO评分恶化情况的AUC从0.68提高到0.78(P=0.0097)和0.75(P=0.021),尽管对于死亡情况只是临界显著。验证队列的结果得到了证实。
这份首份Crit-COV-U报告证明了这样一个概念,即尿液蛋白质组分析能够生成指示COVID-19不良结局的生物标志物,即使在疾病早期阶段,包括WHO的1-3期。这些发现需要在即将到来的最终数据集中得到巩固。
德国联邦卫生部资助了这项研究。