Non-Profit Research Institute Alliance for the Promotion of Preventive Medicine, Mechelen, Belgium; Biomedical Sciences Group, Faculty of Medicine, University of Leuven, Leuven, Belgium.
Department of Infectious Diseases and Tropical Medicine, Nephrology and Kuratorium für Dialyse und Nierentransplantation Renal Unit and Rheumatology, St Georg Hospital, Leipzig, Germany.
Lancet Digit Health. 2022 Oct;4(10):e727-e737. doi: 10.1016/S2589-7500(22)00150-9. Epub 2022 Aug 31.
The SARS-CoV-2 pandemic is a worldwide challenge. The CRIT-CoV-U pilot study generated a urinary proteomic biomarker consisting of 50 peptides (COV50), which predicted death and disease progression from SARS-CoV-2. After the interim analysis presented for the German Government, here, we aimed to analyse the full dataset to consolidate the findings and propose potential clinical applications of this biomarker.
CRIT-CoV-U was a prospective multicentre cohort study. In eight European countries (Austria, France, Germany, Greece, North Macedonia, Poland, Spain, and Sweden), 1012 adults with PCR-confirmed COVID-19 were followed up for death and progression along the 8-point WHO scale. Capillary electrophoresis coupled with mass spectrometry was used for urinary proteomic profiling. Statistical methods included logistic regression and receiver operating characteristic curve analysis with a comparison of the area under curve (AUC) between nested models. Hospitalisation costs were derived from the care facility corresponding with the Markov chain probability of reaching WHO scores ranging from 3 to 8 and flat-rate hospitalisation costs adjusted for the gross per capita domestic product of each country.
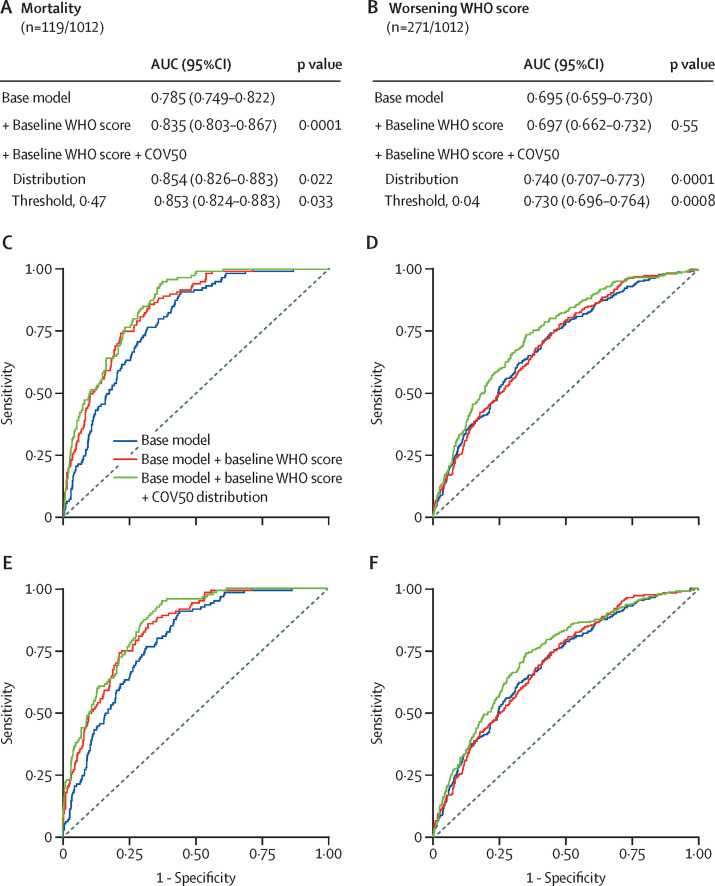
From June 30 to Nov 19, 2020, 228 participants were recruited, and from April 30, 2020, to April 14, 2021, 784 participants were recruited, resulting in a total of 1012 participants. The entry WHO scores were 1-3 in 445 (44%) participants, 4-5 in 529 (52%) participants, and 6 in 38 (4%) participants; and of all participants, 119 died and 271 had disease progression. The odds ratio (OR) associated with COV50 in all 1012 participants for death was 2·44 (95% CI 2·05-2·92) unadjusted and 1·67 (1·34-2·07) when adjusted for sex, age, BMI, comorbidities, and baseline WHO score; and for disease progression, the OR was 1·79 (1·60-2·01) when unadjusted and 1·63 (1·41-1·91) when adjusted (p<0·0001 for all). The predictive accuracy of the optimised COV50 thresholds was 74·4% (71·6-77·1%) for mortality (threshold 0·47) and 67·4% (64·4-70·3%) for disease progression (threshold 0·04). When adjusted for covariables and the baseline WHO score, these thresholds improved AUCs from 0·835 to 0·853 (p=0·033) for death and from 0·697 to 0·730 (p=0·0008) for progression. Of 196 participants who received ambulatory care, 194 (99%) did not reach the 0·04 threshold. The cost reductions associated with 1 day less hospitalisation per 1000 participants were million Euro (M€) 0·887 (5-95% percentile interval 0·730-1·039) in participants at a low risk (COV50 <0·04) and M€2·098 (1·839-2·365) in participants at a high risk (COV50 ≥0·04).
The urinary proteomic COV50 marker might be predictive of adverse COVID-19 outcomes. Even in people with mild-to-moderate PCR-confirmed infections (WHO scores 1-4), the 0·04 COV50 threshold justifies earlier drug treatment, thereby potentially reducing the number of days in hospital and associated costs.
German Federal Ministry of Health.
SARS-CoV-2 大流行是一项全球性挑战。CRIT-CoV-U 试点研究生成了由 50 个肽(COV50)组成的尿蛋白组生物标志物,该标志物可预测 SARS-CoV-2 导致的死亡和疾病进展。在为德国政府进行中期分析后,在此,我们旨在分析完整数据集,以巩固这些发现,并提出该生物标志物的潜在临床应用。
CRIT-CoV-U 是一项前瞻性多中心队列研究。在奥地利、法国、德国、希腊、北马其顿、波兰、西班牙和瑞典等 8 个欧洲国家,对 1012 名 PCR 确诊的 COVID-19 成年患者进行了随访,以了解其死亡和沿 WHO 8 分制进展的情况。毛细管电泳-质谱联用技术用于尿蛋白组学分析。统计方法包括逻辑回归和接收者操作特征曲线分析,比较嵌套模型的曲线下面积(AUC)。根据达到 WHO 评分 3-8 分的马尔可夫链概率和按每个国家人均国内生产总值调整的固定住院费用,得出住院费用。
从 2020 年 6 月 30 日至 11 月 19 日,共招募了 228 名参与者,从 2020 年 4 月 30 日至 2021 年 4 月 14 日,共招募了 784 名参与者,总计 1012 名参与者。入组时的 WHO 评分分别为 1-3 分的有 445 名(44%)患者,4-5 分的有 529 名(52%)患者,6 分的有 38 名(4%)患者;所有患者中,119 人死亡,271 人病情进展。COV50 在所有 1012 名患者中的死亡比值比(OR)为 2.44(95%CI 2.05-2.92),未调整性别、年龄、BMI、合并症和基线 WHO 评分时为 1.67(1.34-2.07);疾病进展时,未调整的 OR 为 1.79(1.60-2.01),调整后的 OR 为 1.63(1.41-1.91)(所有 p<0.0001)。优化后的 COV50 阈值的预测准确性为死亡率的 74.4%(71.6-77.1%)(阈值 0.47)和疾病进展的 67.4%(64.4-70.3%)(阈值 0.04)。当调整协变量和基线 WHO 评分时,这些阈值使死亡率的 AUC 从 0.835 提高到 0.853(p=0.033),疾病进展的 AUC 从 0.697 提高到 0.730(p=0.0008)。在接受门诊治疗的 196 名患者中,194 名(99%)未达到 0.04 阈值。每 1000 名患者减少 1 天住院时间可节省的费用为百万欧元(M€)0.887(5-95%分位数区间 0.730-1.039),在低风险(COV50 <0.04)患者中,M€2.098(1.839-2.365)在高风险(COV50 ≥0.04)患者中。
尿蛋白组 COV50 标志物可能是 COVID-19 不良结局的预测指标。即使在 PCR 确诊的感染程度较轻至中度(WHO 评分 1-4)的患者中,0.04 的 COV50 阈值也支持更早的药物治疗,从而可能减少住院天数和相关费用。
德国联邦卫生部。