Sammartino Daniel, Jafri Farrukh, Cook Brennan, La Lisa, Kim Hyemin, Cardasis John, Raff Joshua
White Plains Hospital, White Plains, New York, United States of America.
Rutgers Robert Wood Johnson School of Medicine, New Brunswick, New Jersey, United States of America.
PLoS One. 2021 May 10;16(5):e0251262. doi: 10.1371/journal.pone.0251262. eCollection 2021.
The coronavirus disease 2019 (COVID-19) pandemic overwhelmed healthcare systems, highlighting the need to better understand predictors of mortality and the impact of medical interventions.
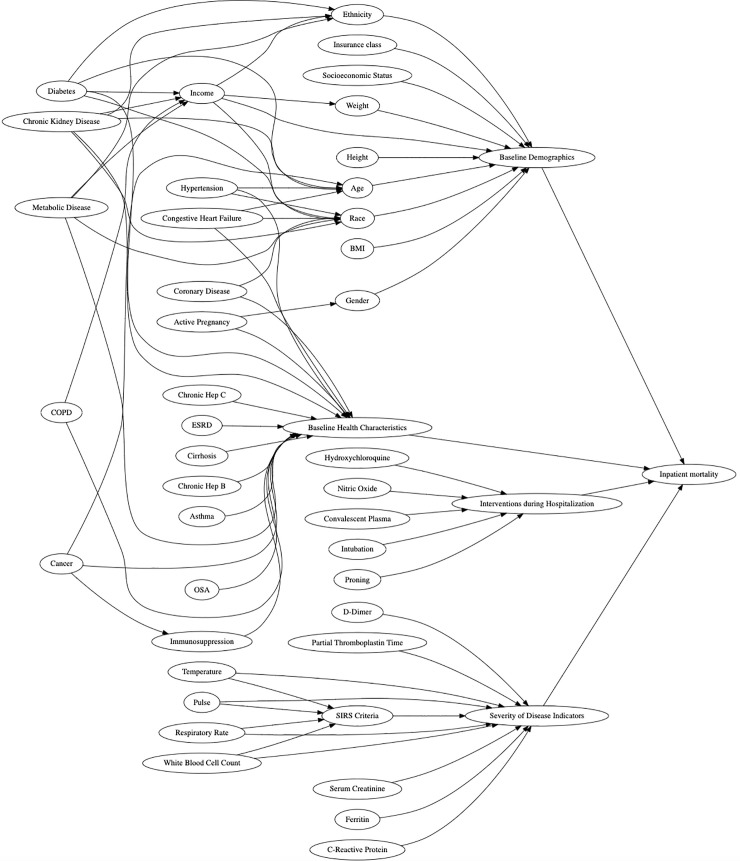
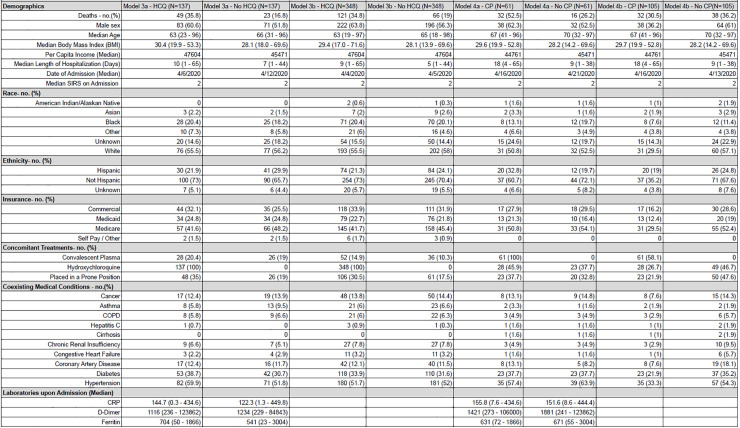
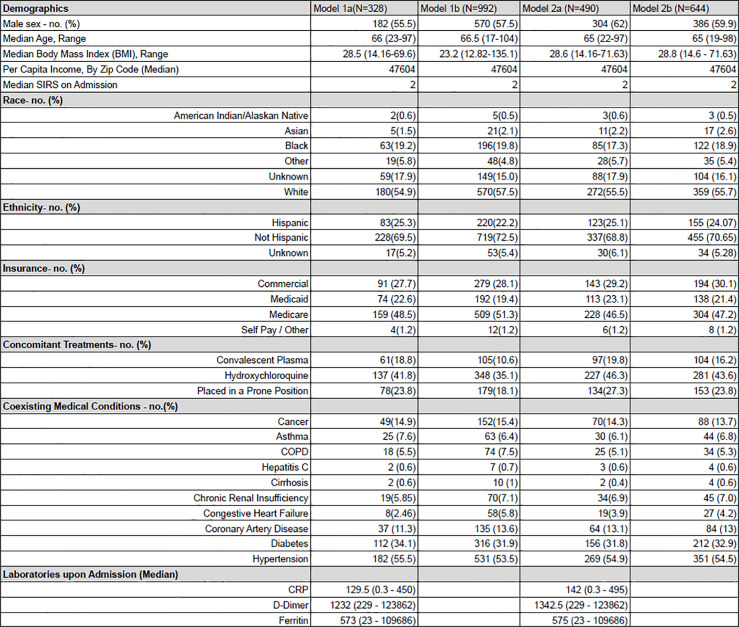
This retrospective cohort study examined data from every patient who tested positive for COVID-19 and was admitted to White Plains Hospital between March 9, 2020, and June 3, 2020. We used binomial logistic regression to analyze data for all patients, and propensity score matching for those treated with hydroxychloroquine and convalescent plasma (CP). The primary outcome of interest was inpatient mortality.
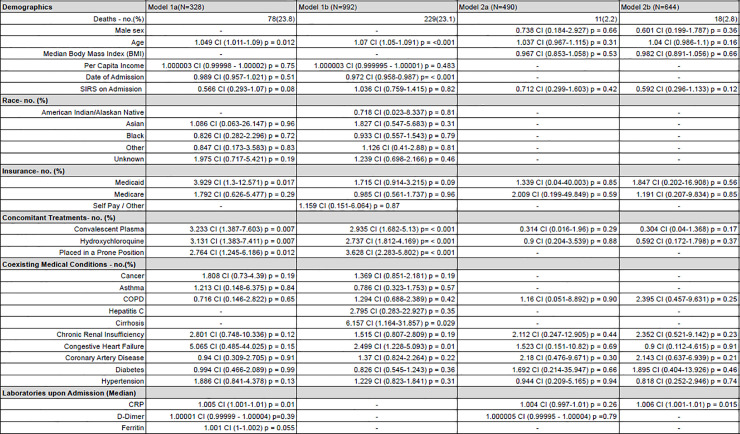
1,108 admitted patients with COVID-19 were available for analysis, of which 124 (11.2%) were excluded due to incomplete data. Of the 984 patients included, 225 (22.9%) died. Risk for death decreased for each day later a patient was admitted [OR 0.970, CI 0.955 to 0.985; p < 0.001]. Elevated initial C-reactive protein (CRP) value was associated with a higher risk for death at 96 hours [OR 1.007, 1.002 to 1.012; p = 0.006]. Hydroxychloroquine and CP administration were each associated with increased mortality [OR 3.4, CI 1.614 to 7.396; p = 0.002, OR 2.8560, CI 1.361 to 6.160; p = 0.006 respectively].
Elevated CRP carried significant odds of early death. Hydroxychloroquine and CP were each associated with higher risk for death, although CP was without titers and was administered at a median of five days from admission. Randomized or controlled studies will better describe the impact of CP. Mortality decreased as the pandemic progressed, suggesting that institutional capacity for dynamic evaluation of process and outcome measures may benefit COVID-19 survival.
2019年冠状病毒病(COVID-19)大流行使医疗系统不堪重负,凸显了更好地了解死亡率预测因素以及医学干预措施影响的必要性。
这项回顾性队列研究分析了2020年3月9日至2020年6月3日期间在白原医院检测出COVID-19呈阳性并入院的每一位患者的数据。我们使用二项逻辑回归分析所有患者的数据,并对接受羟氯喹和康复期血浆(CP)治疗的患者进行倾向得分匹配。主要关注的结局是住院死亡率。
1108例COVID-19住院患者可供分析,其中124例(11.2%)因数据不完整被排除。在纳入的984例患者中,225例(22.9%)死亡。患者入院时间每推迟一天,死亡风险降低[比值比(OR)0.970,置信区间(CI)0.955至0.985;p<0.001]。初始C反应蛋白(CRP)值升高与96小时时较高的死亡风险相关[OR 1.007,1.002至1.012;p = 0.006]。羟氯喹和CP治疗均与死亡率增加相关[OR 3.4,CI 1.614至7.396;p = 0.002,OR 2.8560,CI 1.361至6.160;p = 0.006]。
CRP升高具有早期死亡的显著几率。羟氯喹和CP均与较高的死亡风险相关,尽管CP没有效价且给药时间中位数为入院后五天。随机或对照研究将更好地描述CP的影响。随着大流行的进展,死亡率下降,这表明对过程和结局指标进行动态评估的机构能力可能有利于COVID-19患者存活。