Calligaro Gregory L, Lalla Usha, Audley Gordon, Gina Phindile, Miller Malcolm G, Mendelson Marc, Dlamini Sipho, Wasserman Sean, Meintjes Graeme, Peter Jonathan, Levin Dion, Dave Joel A, Ntusi Ntobeko, Meier Stuart, Little Francesca, Moodley Desiree L, Louw Elizabeth H, Nortje Andre, Parker Arifa, Taljaard Jantjie J, Allwood Brian W, Dheda Keertan, Koegelenberg Coenraad F N
Centre for Lung Infection and Immunity, Division of Pulmonology, Department of Medicine and UCT Lung Institute and South African MRC/UCT Centre for the Study of Antimicrobial Resistance, University of Cape Town, Cape Town, South Africa.
Division of Critical Care, Department of Anaesthesia and Perioperative Medicine, University of Cape Town and Groote Schuur Hospital, Cape Town, South Africa.
EClinicalMedicine. 2020 Nov;28:100570. doi: 10.1016/j.eclinm.2020.100570. Epub 2020 Oct 6.
The utility of heated and humidified high-flow nasal oxygen (HFNO) for severe COVID-19-related hypoxaemic respiratory failure (HRF), particularly in settings with limited access to intensive care unit (ICU) resources, remains unclear, and predictors of outcome have been poorly studied.
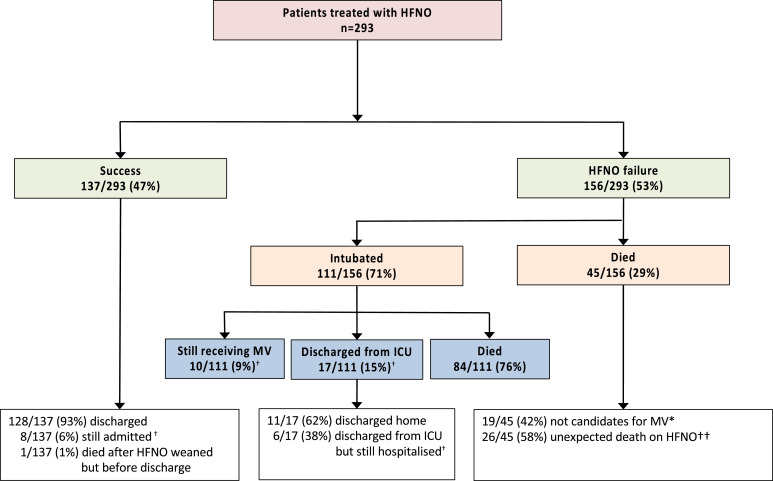
We included consecutive patients with COVID-19-related HRF treated with HFNO at two tertiary hospitals in Cape Town, South Africa. The primary outcome was the proportion of patients who were successfully weaned from HFNO, whilst failure comprised intubation or death on HFNO.
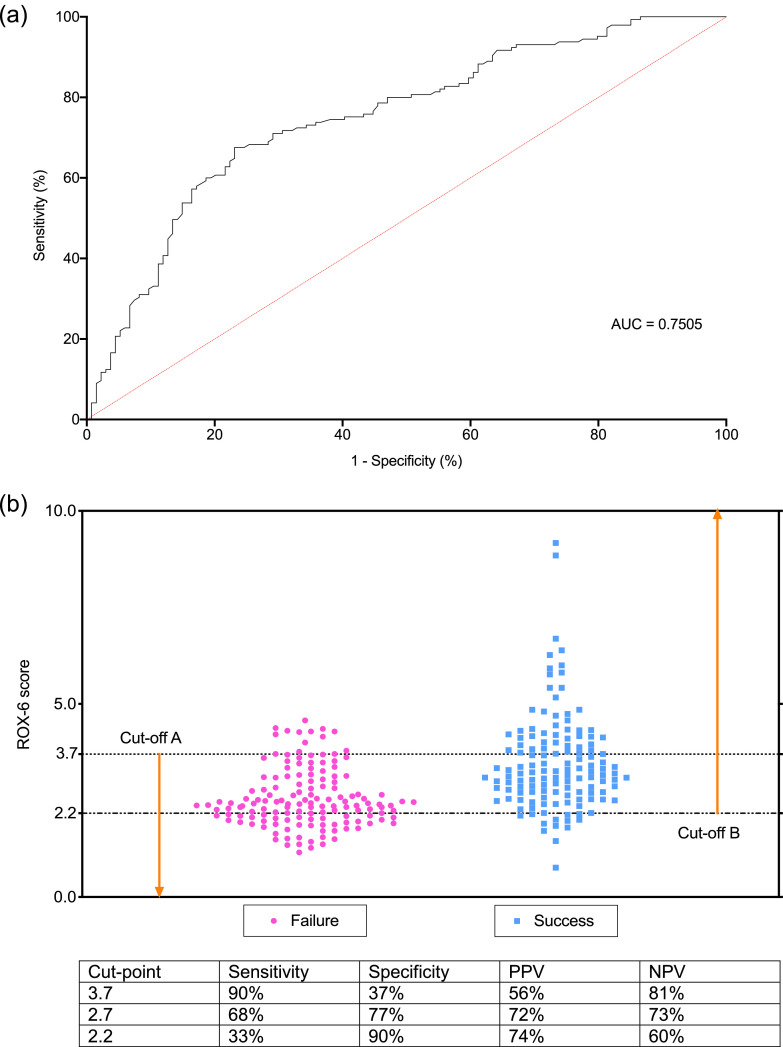
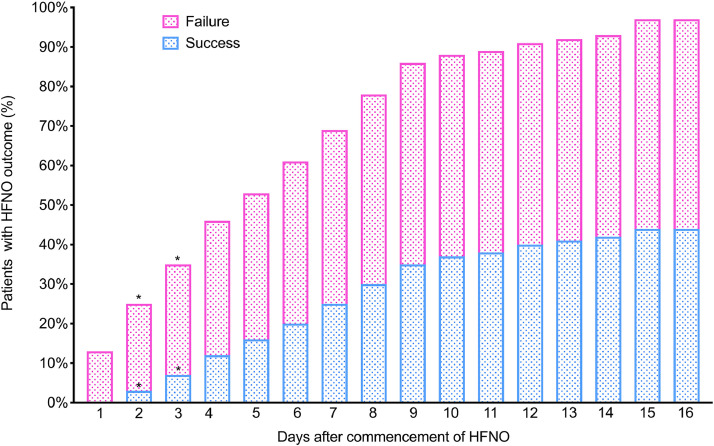
The median (IQR) arterial oxygen partial pressure to fraction inspired oxygen ratio (PO2/FiO) was 68 (54-92) in 293 enroled patients. Of these, 137/293 (47%) of patients [PO2/FiO 76 (63-93)] were successfully weaned from HFNO. The median duration of HFNO was 6 (3-9) in those successfully treated versus 2 (1-5) days in those who failed (<0.001). A higher ratio of oxygen saturation/FiO2 to respiratory rate within 6 h (ROX-6 score) after HFNO commencement was associated with HFNO success (ROX-6; AHR 0.43, 0.31-0.60), as was use of steroids (AHR 0.35, 95%CI 0.19-0.64). A ROX-6 score of ≥3.7 was 80% predictive of successful weaning whilst ROX-6 ≤ 2.2 was 74% predictive of failure. In total, 139 patents (52%) survived to hospital discharge, whilst mortality amongst HFNO failures with outcomes was 129/140 (92%).
In a resource-constrained setting, HFNO for severe COVID-19 HRF is feasible and more almost half of those who receive it can be successfully weaned without the need for mechanical ventilation.
对于严重新型冠状病毒肺炎(COVID-19)相关的低氧性呼吸衰竭(HRF),尤其是在重症监护病房(ICU)资源有限的情况下,使用加热湿化高流量鼻导管给氧(HFNO)的效果仍不明确,且对预后预测因素的研究较少。
我们纳入了南非开普敦两家三级医院中接受HFNO治疗的COVID-19相关HRF连续患者。主要结局是成功停用HFNO的患者比例,而治疗失败包括在使用HFNO期间进行气管插管或死亡。
293例纳入患者的动脉血氧分压与吸入氧分数比(PO2/FiO)的中位数(IQR)为68(54-92)。其中,137/293(47%)的患者[PO2/FiO 76(63-93)]成功停用HFNO。成功治疗患者的HFNO中位持续时间为6(3-9)天,而治疗失败患者为2(1-5)天(<0.001)。HFNO开始后6小时内较高的氧饱和度/FiO2与呼吸频率之比(ROX-6评分)与HFNO治疗成功相关(ROX-6;风险比0.43,0.31-0.60),使用类固醇也是如此(风险比0.35,95%置信区间0.19-0.64)。ROX-6评分≥3.7对成功撤机的预测准确率为80%,而ROX-6≤2.2对治疗失败的预测准确率为74%。共有139例患者(52%)存活至出院,而HFNO治疗失败且有结局患者的死亡率为129/140(92%)。
在资源有限的情况下,HFNO用于治疗严重COVID-19 HRF是可行的,近一半接受该治疗的患者无需机械通气即可成功撤机。