Department of Public Health, Erasmus MC University Medical Center Rotterdam, the Netherlands.
Program in Computational Biology, Fred Hutchinson Cancer Research Center, Seattle, Washington.
Gastroenterology. 2021 Aug;161(2):487-494.e4. doi: 10.1053/j.gastro.2021.05.003. Epub 2021 May 8.
Current guidelines recommend surveillance for patients with nondysplastic Barrett's esophagus (NDBE) but do not include a recommended age for discontinuing surveillance. This study aimed to determine the optimal age for last surveillance of NDBE patients stratified by sex and level of comorbidity.
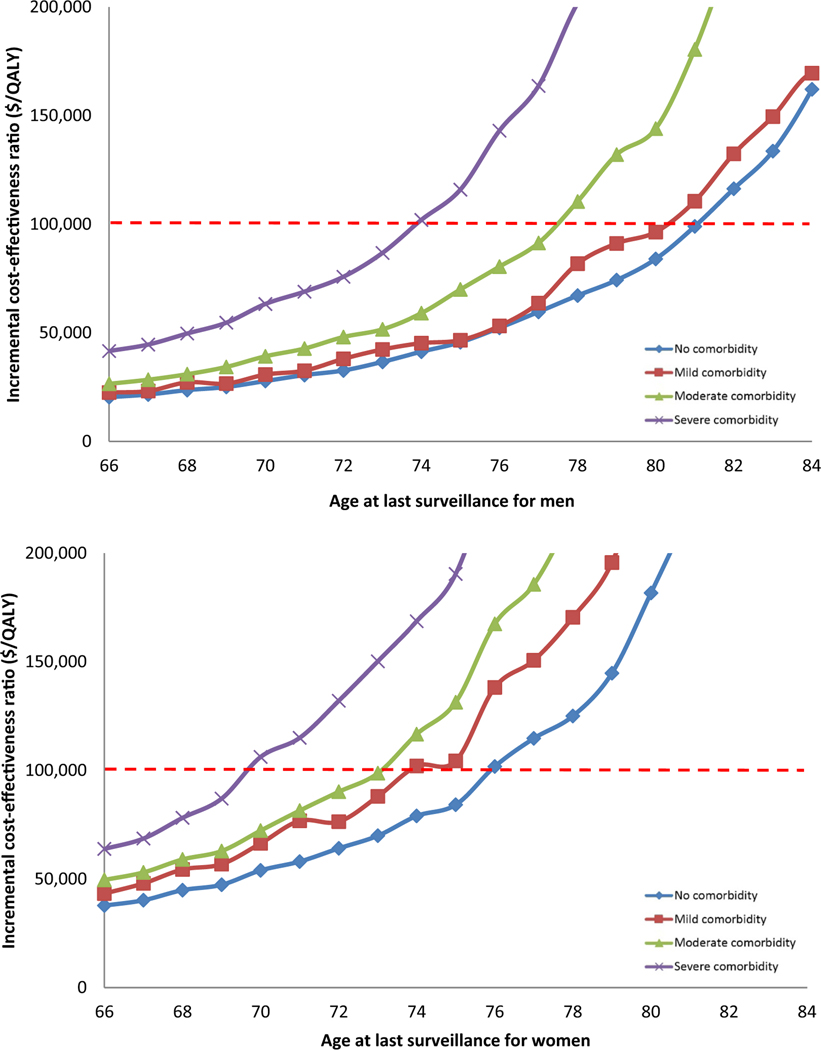
We used 3 independently developed models to simulate patients diagnosed with NDBE, varying in age, sex, and comorbidity level (no, mild, moderate, and severe). All patients had received regular surveillance until their current age. We calculated incremental costs and quality-adjusted life-years (QALYs) gained from 1 additional endoscopic surveillance at the current age versus not performing surveillance at that age. We determined the optimal age to end surveillance as the age at which incremental cost-effectiveness ratio of 1 more surveillance was just less than the willingness-to-pay threshold of $100,000/QALY.
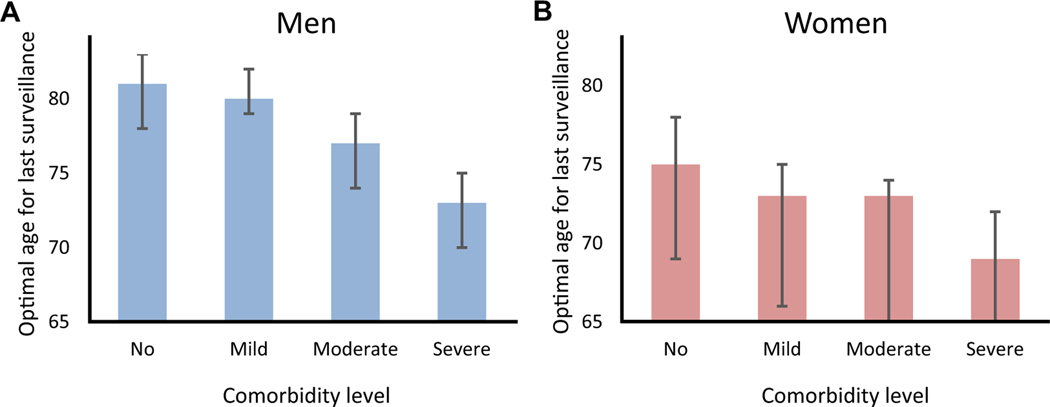
The benefit of having 1 more surveillance endoscopy strongly depended on age, sex, and comorbidity. For men with NDBE and severe comorbidity, 1 additional surveillance at age 80 years provided 4 more QALYs per 1000 patients with BE at an additional cost of $1.2 million, whereas for women with severe comorbidity the benefit at that age was 7 QALYs at a cost of $1.3 million. For men with no, mild, moderate, and severe comorbidity, the optimal ages of last surveillance were 81, 80, 77, and 73 years, respectively. For women, these ages were younger: 75, 73, 73, and 69 years, respectively.
Our comparative modeling analysis illustrates the importance of considering comorbidity status and sex when deciding on the age to discontinue surveillance in patients with NDBE.
目前的指南建议对非异型性 Barrett 食管(NDBE)患者进行监测,但不包括停止监测的建议年龄。本研究旨在确定根据性别和合并症水平分层的 NDBE 患者最后一次进行 NDBE 监测的最佳年龄。
我们使用 3 个独立开发的模型来模拟年龄、性别和合并症水平(无、轻度、中度和重度)不同的 NDBE 患者。所有患者均接受了定期监测,直至当前年龄。我们计算了从当前年龄进行 1 次额外内镜监测与不进行该年龄监测相比,增加的成本和获得的质量调整生命年(QALY)。我们将结束监测的最佳年龄定义为每增加 1 次监测的增量成本效益比刚刚低于 10 万美元/QALY 的意愿支付阈值的年龄。
进行 1 次额外内镜监测的获益强烈取决于年龄、性别和合并症。对于患有 NDBE 和严重合并症的男性,80 岁时进行 1 次额外监测可使每 1000 例 BE 患者多获得 4 个 QALY,额外费用为 120 万美元,而对于严重合并症的女性,该年龄的获益为 7 个 QALY,成本为 130 万美元。对于无、轻度、中度和重度合并症的男性,最后监测的最佳年龄分别为 81、80、77 和 73 岁。对于女性,这些年龄则更年轻:分别为 75、73、73 和 69 岁。
我们的比较建模分析表明,在决定停止 NDBE 患者监测的年龄时,需要考虑合并症状况和性别。