Laboratory of Inflammatory Skin Diseases, Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, New York; Department of Dermatology, University Hospital Zürich, Zürich, Switzerland.
Laboratory of Inflammatory Skin Diseases, Department of Dermatology, Icahn School of Medicine at Mount Sinai, New York, New York; Laboratory for Investigative Dermatology, The Rockefeller University, New York, New York.
Ann Allergy Asthma Immunol. 2021 Sep;127(3):334-341. doi: 10.1016/j.anai.2021.04.023. Epub 2021 May 9.
Atopic dermatitis (AD) is a common disease, with particularly high prevalence found in Africa. It is increasingly recognized that patients with AD of different ethnic backgrounds have unique molecular signatures in the skin, potentially accounting for treatment response variations. Nevertheless, the skin profile of patients with AD from Africa is unknown, hindering development of new treatments targeted to this patient population.
To characterize the skin profile of patients with AD from Africa.
Gene expression studies, including RNA sequencing (using threshold of fold change of >2 and false discovery rate of <0.05) and real-time polymerase chain reaction, were performed on skin biopsies of Tanzanian patients with moderate-to-severe AD and controls.
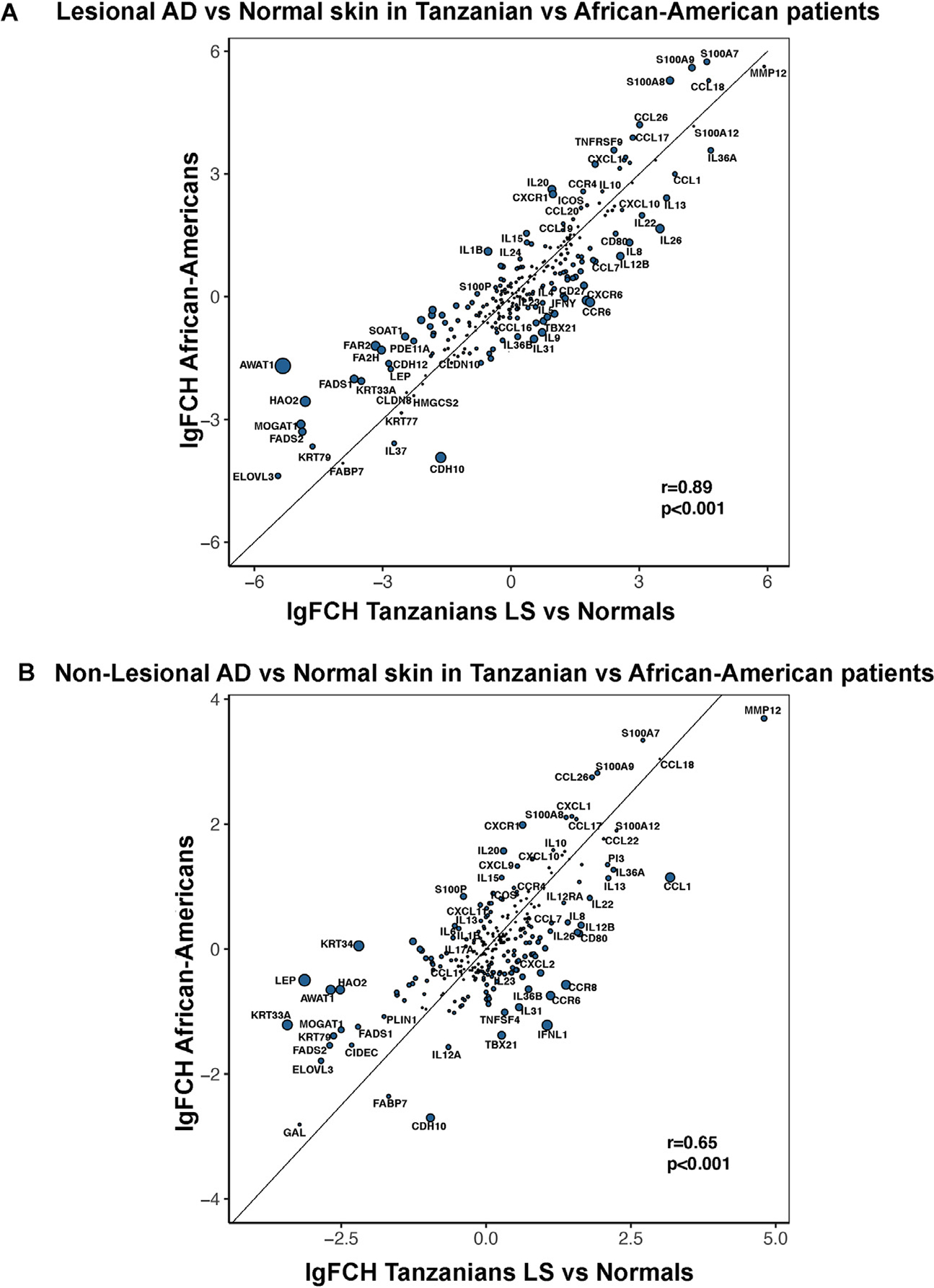
Tanzanian AD skin presented robust up-regulations of multiple key mediators of both T helper 2 (T2) (interleukin 13 [IL-13], IL-10, IL-4R, CCL13,CCL17,CCL18,CCL26) and T22 (IL22, S100As) pathways. Markers related to T17 and IL-23 (IL-17A, IL-23A, IL-12, PI3, DEFB4B) and T1 (interferon gamma, CXCL9,CXCL10,CXCL11) were also significantly overexpressed in AD tissues (FDR<.05), albeit to a lesser extent. IL-36 isoforms revealed substantial up-regulations in African skin. The barrier fingerprint of Tanzanian AD revealed no suppression of hallmark epidermal barrier differentiation genes, such as filaggrin, loricrin, and periplakin, with robust attenuation of lipid metabolism genes (ie, AWAT1).
The skin phenotype of Tanzanian patients with AD is consistent with that of African Americans, exhibiting dominant T2 and T22 skewing, minimal dysregulation of terminal differentiation, and even broader attenuation of lipid metabolism-related products. These data highlight the unique characteristic of AD in Black individuals and the need to develop unique treatments targeting patients with AD from these underrepresented populations.
特应性皮炎(AD)是一种常见疾病,在非洲的发病率尤其高。人们越来越认识到,不同种族背景的 AD 患者的皮肤具有独特的分子特征,这可能导致治疗反应的差异。然而,非洲 AD 患者的皮肤特征尚不清楚,这阻碍了针对这一患者群体的新疗法的开发。
描述来自非洲的 AD 患者的皮肤特征。
对坦桑尼亚中重度 AD 患者和对照者的皮肤活检组织进行了基因表达研究,包括 RNA 测序(采用倍数变化>2 和假发现率<0.05 的阈值)和实时聚合酶链反应。
坦桑尼亚 AD 皮肤呈现出多个 T 辅助 2(T2)(白细胞介素 13[IL-13]、IL-10、IL-4R、CCL13、CCL17、CCL18、CCL26)和 T22(IL22、S100As)通路关键介质的显著上调。T17 和 IL-23(IL-17A、IL-23A、IL-12、PI3、DEFB4B)和 T1(干扰素γ、CXCL9、CXCL10、CXCL11)途径的标志物在 AD 组织中也显著过表达(FDR<0.05),尽管程度较轻。IL-36 同种型在非洲皮肤中呈现出显著的上调。坦桑尼亚 AD 的屏障特征指纹显示,标志性的表皮屏障分化基因(如丝聚蛋白、兜甲蛋白和桥粒芯糖蛋白)没有受到抑制,而脂质代谢基因(如 AWAT1)则受到强烈抑制。
坦桑尼亚 AD 患者的皮肤表型与非裔美国人一致,表现出主导的 T2 和 T22 偏倚,终端分化的轻微失调,甚至更广泛的脂质代谢相关产物的抑制。这些数据突出了黑人个体中 AD 的独特特征,以及针对这些代表性不足的患者群体开发独特治疗方法的必要性。