Division of Trauma, Emergency Surgery and Surgical Critical Care, Massachusetts General Hospital, Boston, Massachusetts.
Division of Trauma, Emergency Surgery and Surgical Critical Care, Massachusetts General Hospital, Boston, Massachusetts.
J Surg Res. 2021 Oct;266:35-43. doi: 10.1016/j.jss.2021.03.049. Epub 2021 Apr 6.
Bedside experience and studies of critically ill patients with coronavirus disease 2019 (COVID-19) indicate COVID-19 to be a devastating multisystem disease. We aim to describe the incidence, associated variables, and outcomes of rhabdomyolysis in critically ill COVID-19 patients.
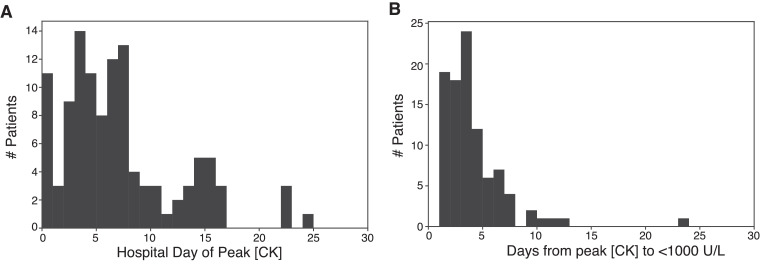
Data for all critically ill adult patients (≥18 years old) admitted to the ICU at a large academic medical center with confirmed COVID-19 between March 13, 2020 and April 18, 2020 were prospectively collected. Patients with serum creatine kinase (CK) concentrations greater than 1000 U/L were diagnosed with rhabdomyolysis. Patients were further stratified as having moderate (serum CK concentration 1000-4999 U/L) or severe (serum CK concentration ≥5000 U/L) rhabdomyolysis. Univariate and multivariate analyses were performed to identify outcomes and variables associated with the development of rhabdomyolysis.
Of 235 critically ill COVID-19 patients, 114 (48.5%) met diagnostic criteria for rhabdomyolysis. Patients with rhabdomyolysis more often required mechanical ventilation (P < 0.001), prone positioning (P < 0.001), pharmacological paralysis (P < 0.001), renal replacement therapy (P = 0.010), and extracorporeal membrane oxygenation (ECMO) (P = 0.025). They also had longer median ICU length of stay (LOS) (P < 0.001) and hospital LOS (P < 0.001). No difference in mortality was observed. Male sex, patients with morbid obesity, SOFA score, and prone positioning were independently associated with rhabdomyolysis.
Nearly half of critically ill COVID-19 patients in our cohort met diagnostic criteria for rhabdomyolysis. Male sex, morbid obesity, SOFA score, and prone position were independently associated with rhabdomyolysis.
对患有 2019 年冠状病毒病(COVID-19)的危重症患者的床边经验和研究表明,COVID-19 是一种破坏性的多系统疾病。我们旨在描述危重症 COVID-19 患者横纹肌溶解症的发生率、相关变量和结局。
2020 年 3 月 13 日至 4 月 18 日期间,前瞻性收集了一家大型学术医疗中心 ICU 收治的所有确诊 COVID-19 的成年危重症患者(≥18 岁)的数据。血清肌酸激酶(CK)浓度大于 1000 U/L 的患者被诊断为横纹肌溶解症。患者进一步分为中度(血清 CK 浓度 1000-4999 U/L)或重度(血清 CK 浓度≥5000 U/L)横纹肌溶解症。进行单变量和多变量分析以确定与横纹肌溶解症发生相关的结局和变量。
在 235 例危重症 COVID-19 患者中,114 例(48.5%)符合横纹肌溶解症的诊断标准。横纹肌溶解症患者更常需要机械通气(P < 0.001)、俯卧位(P < 0.001)、药物性麻痹(P < 0.001)、肾脏替代治疗(P = 0.010)和体外膜肺氧合(ECMO)(P = 0.025)。他们的 ICU 中位住院时间(LOS)(P < 0.001)和医院 LOS 也更长。死亡率无差异。男性、病态肥胖、SOFA 评分和俯卧位是横纹肌溶解症的独立相关因素。
在我们的研究队列中,近一半的危重症 COVID-19 患者符合横纹肌溶解症的诊断标准。男性、病态肥胖、SOFA 评分和俯卧位与横纹肌溶解症独立相关。