Adult Intensive Care Unit, Hospital Sírio-Libanês, São Paulo, Brazil.
Research and Education Institute, Hospital Sírio-Libanês, São Paulo, Brazil.
PLoS One. 2020 Dec 3;15(12):e0243269. doi: 10.1371/journal.pone.0243269. eCollection 2020.
The coronavirus disease (COVID-19) pandemic has brought significant challenges worldwide, with high mortality, increased use of hospital resources, and the collapse of healthcare systems. We aimed to describe the clinical outcomes of critically ill COVID-19 patients and assess the impact on the use of hospital resources and compare with critically ill medical patients without COVID-19.
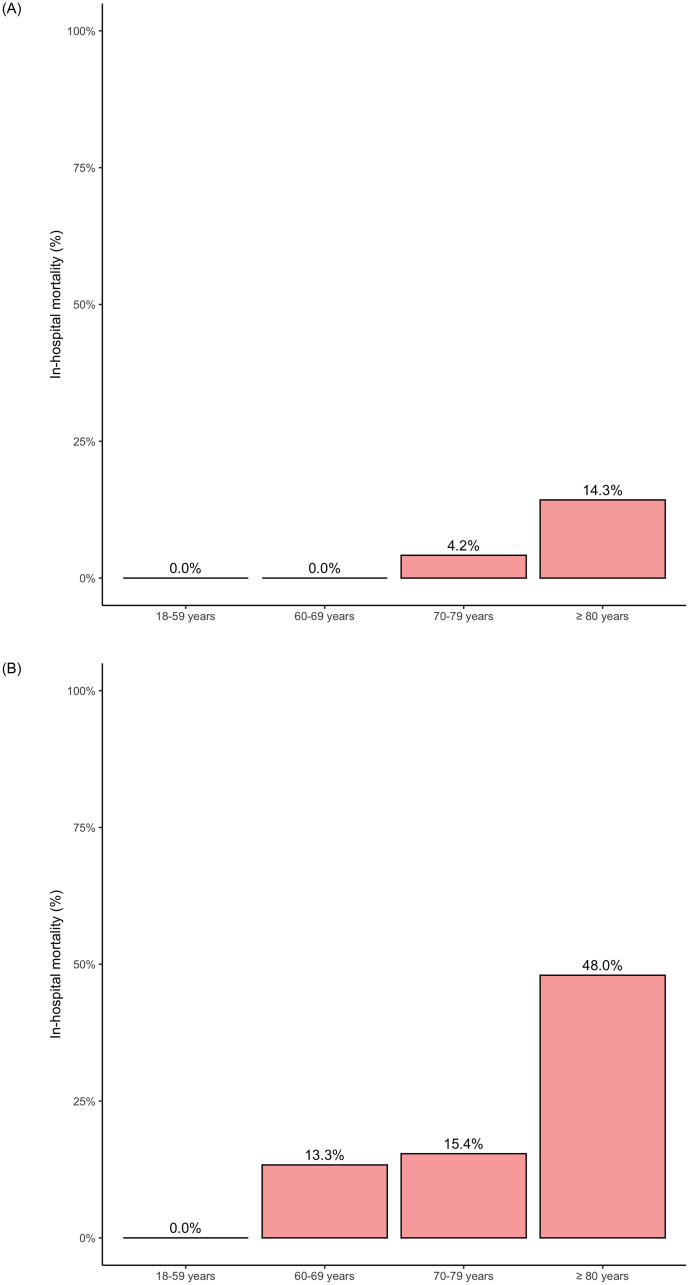
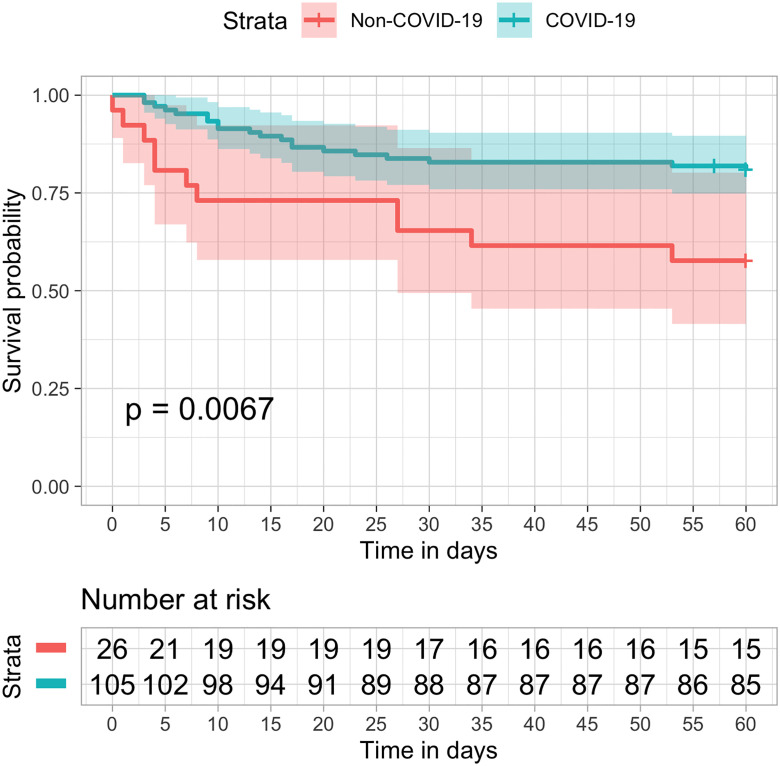
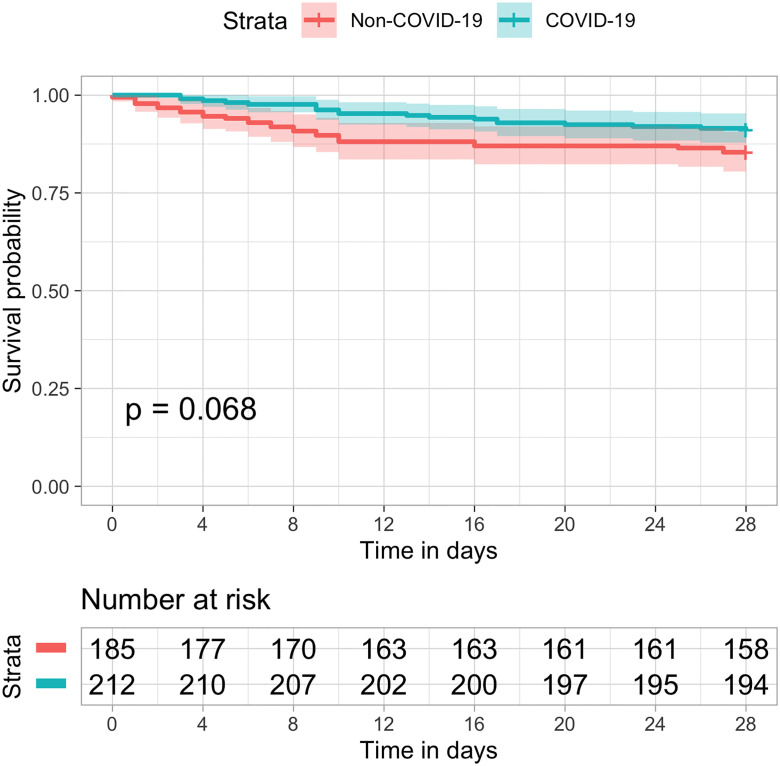
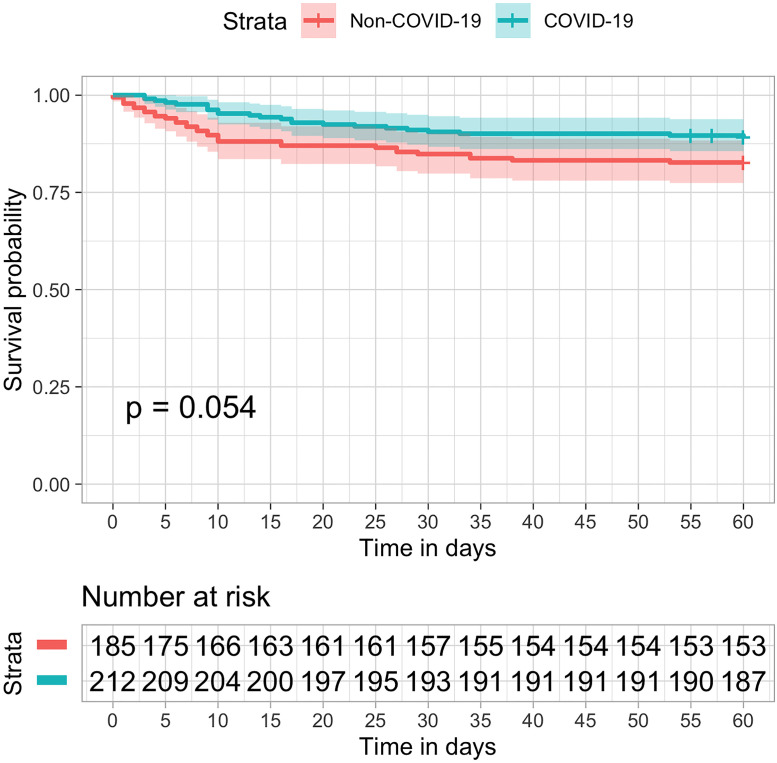
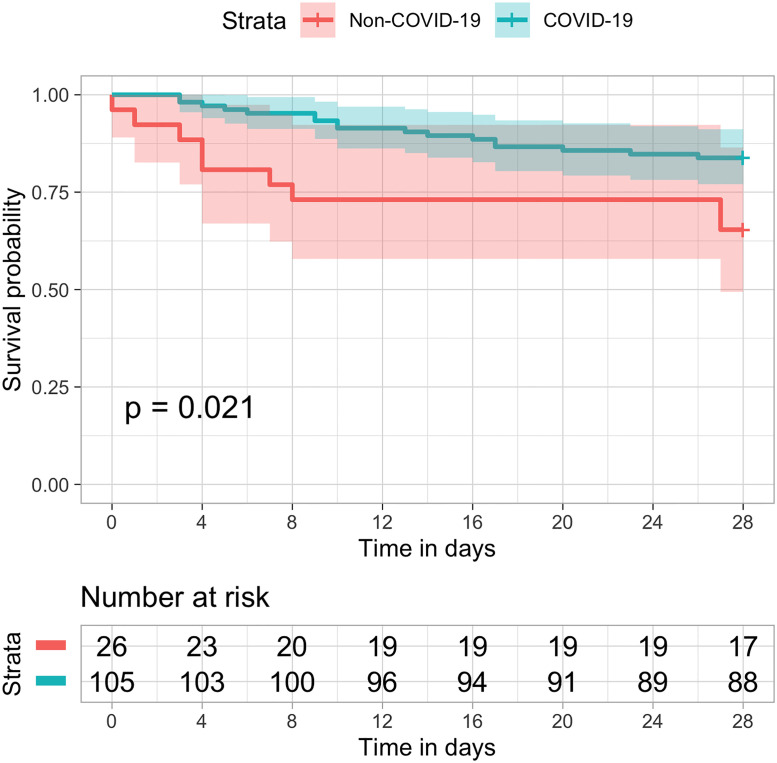
In this retrospective cohort study, we included patients diagnosed with COVID-19 admitted to a private ICU in Sao Paulo, Brazil from March to June 2020. We compared these patients with those admitted to the unit in the same period of the previous year. A total of 212 consecutive patients with a confirmed diagnosis of COVID-19 were compared with 185 medical patients from the previous year. Patients with COVID-19 were more frequently males (76% vs. 56%, p<0.001) and morbidly obese (7.5% vs. 2.2%, p = 0.027), and had lower SAPS 3 (49.65 (12.19) vs. 55.63 (11.94), p<0.001) and SOFA scores (3.78 (3.53) vs. 4.48 (3.11), p = 0.039). COVID-19 patients had a longer ICU stay (median of 7 vs. 3 days, p<0.001), longer duration of mechanical ventilation (median of 9 vs. 4 days, p = 0.003), and more frequent tracheostomies (10.8 vs. 1.1%, p<0.001). Survival rates until 28 days were not statistically different (91% vs. 85.4%, p = 0.111). After multivariable adjustment for age, gender, SAPS 3, and Charlson Comorbidity Index, COVID-19 remained not associated with survival at 28 days (HR 0.59, 95% CI 0.33-1.06, p = 0.076). Among patients who underwent invasive mechanical ventilation, the observed mortality at 28-days was 16.2% in COVID-19 patients compared to 34.6% in the previous year.
COVID-19 required more hospital resources, including invasive and non-invasive ventilation, had a longer duration of mechanical ventilation, and a more prolonged ICU and hospital length of stay. There was no difference in all-cause mortality at 28 and 60 days, suggesting that health systems preparedness be an important determinant of clinical outcomes.
冠状病毒病(COVID-19)大流行给全球带来了巨大挑战,病死率高,医院资源使用增加,医疗体系崩溃。我们旨在描述重症 COVID-19 患者的临床结局,并评估对医院资源使用的影响,并与无 COVID-19 的重症内科患者进行比较。
在这项回顾性队列研究中,我们纳入了 2020 年 3 月至 6 月期间在巴西圣保罗一家私立 ICU 确诊为 COVID-19 并收治的患者。我们将这些患者与前一年同期收治的患者进行了比较。共比较了 212 例连续确诊为 COVID-19 的患者与前一年的 185 例内科患者。COVID-19 患者中男性更为常见(76% vs. 56%,p<0.001),病态肥胖更为常见(7.5% vs. 2.2%,p = 0.027),SAPS 3 评分(49.65(12.19) vs. 55.63(11.94),p<0.001)和 SOFA 评分(3.78(3.53) vs. 4.48(3.11),p = 0.039)更低。COVID-19 患者 ICU 入住时间更长(中位数 7 天 vs. 3 天,p<0.001),机械通气时间更长(中位数 9 天 vs. 4 天,p = 0.003),气管切开术更为常见(10.8% vs. 1.1%,p<0.001)。28 天的生存率无统计学差异(91% vs. 85.4%,p = 0.111)。在调整年龄、性别、SAPS 3 和 Charlson 合并症指数后,COVID-19 与 28 天的生存率无关(HR 0.59,95%CI 0.33-1.06,p = 0.076)。在接受有创机械通气的患者中,COVID-19 患者 28 天的死亡率为 16.2%,而前一年为 34.6%。
COVID-19 需要更多的医院资源,包括有创和无创通气,机械通气时间更长,ICU 和住院时间更长。28 天和 60 天的全因死亡率无差异,提示卫生系统准备情况是临床结局的重要决定因素。