Center of Cardiology, Beijing Chaoyang Hospital, Capital Medical University, 5 Jingyuan Road, Beijing, 100043, China.
Sci Rep. 2021 May 11;11(1):9959. doi: 10.1038/s41598-021-89419-6.
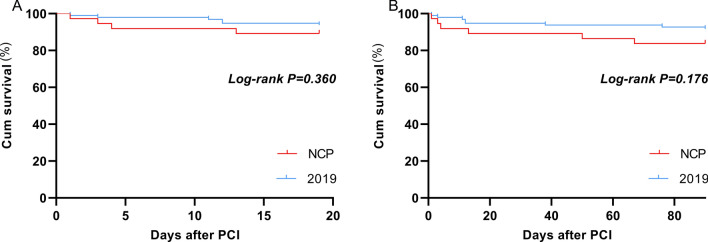
Coronavirus disease 2019 (COVID-19) is a global pandemic impacting nearly 170 countries/regions and millions of patients worldwide. Patients with acute myocardial infarction (AMI) still need to be treated at percutaneous coronary intervention (PCI) centers with relevant safety measures. This retrospective study was conducted to assess the therapeutic outcomes of PCI performed under the safety measures and normal conditions. AMI patients undergoing PCI between January 24 to April 30, 2020 were performed under safety measures for COVID-19. Patients received pulmonary computed tomography (CT) and underwent PCI in negative pressure ICU. Cardiac catheterization laboratory (CCL) staff and physicians worked with level III personal protection. Demographic and clinical data, such as door-to-balloon (DTB) time, operation time, complications for patients in this period (COVID-19 group) and the same period in 2019 (2019 group) were retrieved and analyzed. COVID-19 and 2019 groups had 37 and 96 patients, respectively. There was no significant difference in age, gender, BMI and comorbidity between the two groups. DTB time and operation time were similar between the two groups (60.0 ± 12.39 vs 58.83 ± 12.85 min, p = 0.636; 61.46 ± 9.91 vs 62.55 ± 10.72 min, p = 0.592). Hospital stay time in COVID-19 group was significantly shorter (6.78 ± 2.14 vs 8.85 ± 2.64 days, p < 0.001). The incidences of malignant arrhythmia and Takotsubo Syndrome in COVID-19 group were higher than 2019 group significantly (16.22% vs 5.21%, p = 0.039; 10.81% vs 1.04% p = 0.008). During hospitalization and 3-month follow-up, the incidence of major adverse cardiovascular events and mortality in the two groups were statistically similar (35.13% vs 14.58%, p = 0.094; 16.22% vs 8.33%, p = 0.184). The risk of major adverse cardiac events (MACE) was associated with cardiogenic shock (OR, 11.53; 95% CI, 2.888-46.036; p = 0.001), malignant arrhythmias (OR, 7.176; 95% CI, 1.893-27.203; p = 0.004) and advanced age (≥ 75 years) (OR, 6.718; 95% CI, 1.738-25.964; p = 0.006). Cardiogenic shock (OR, 17.663; 95% CI, 5.5-56.762; p < 0.001) and malignant arrhythmias (OR, 4.659; 95% CI, 1.481-14.653; p = 0.008) were also associated with death of 3 months. Our analysis showed that safety measures undertaken in this hospital, including screening of COVID-19 infection and use of personal protection equipment for conducting PCI did not compromise the surgical outcome as compared with PCI under normal condition, although there were slight increases in incidence of malignant arrhythmia and Takotsubo Syndrome.
新型冠状病毒病 2019(COVID-19)是一种全球大流行疾病,影响了全球近 170 个国家/地区和数以百万计的患者。急性心肌梗死(AMI)患者仍需在具备相关安全措施的经皮冠状动脉介入治疗(PCI)中心进行治疗。本回顾性研究旨在评估在 COVID-19 安全措施下进行 PCI 的治疗效果,并与正常情况下的治疗效果进行比较。2020 年 1 月 24 日至 4 月 30 日期间,AMI 患者在 COVID-19 安全措施下进行 PCI。患者接受肺部计算机断层扫描(CT)检查,并在负压 ICU 中进行 PCI。心脏导管室(CCL)工作人员和医生采用三级个人防护措施进行操作。检索并分析了该时期(COVID-19 组)和 2019 年同期(2019 组)患者的人口统计学和临床数据,如门球时间(DTB)、手术时间、并发症等。COVID-19 组和 2019 组分别有 37 例和 96 例患者。两组患者的年龄、性别、BMI 和合并症无显著差异。两组患者的 DTB 时间和手术时间相似(60.0±12.39 分钟 vs 58.83±12.85 分钟,p=0.636;61.46±9.91 分钟 vs 62.55±10.72 分钟,p=0.592)。COVID-19 组患者的住院时间明显更短(6.78±2.14 天 vs 8.85±2.64 天,p<0.001)。COVID-19 组恶性心律失常和 Takotsubo 综合征的发生率明显高于 2019 组(16.22% vs 5.21%,p=0.039;10.81% vs 1.04%,p=0.008)。在住院期间和 3 个月随访期间,两组患者主要不良心血管事件和死亡率的发生率无统计学差异(35.13% vs 14.58%,p=0.094;16.22% vs 8.33%,p=0.184)。主要不良心脏事件(MACE)的风险与心源性休克(OR,11.53;95%CI,2.888-46.036;p=0.001)、恶性心律失常(OR,7.176;95%CI,1.893-27.203;p=0.004)和高龄(≥75 岁)(OR,6.718;95%CI,1.738-25.964;p=0.006)有关。心源性休克(OR,17.663;95%CI,5.5-56.762;p<0.001)和恶性心律失常(OR,4.659;95%CI,1.481-14.653;p=0.008)也与 3 个月死亡有关。本分析表明,与正常情况下进行 PCI 相比,我院采取的 COVID-19 感染筛查和个人防护设备使用等安全措施并未影响手术结果,但恶性心律失常和 Takotsubo 综合征的发生率略有增加。