Spraider Patrick, Putzer Gabriel, Breitkopf Robert, Abram Julia, Mathis Simon, Glodny Bernhard, Martini Judith
Department of Anaesthesiology and Intensive Care Medicine, Medical University Innsbruck, Innsbruck, Austria.
Department of Radiology, Medical University Innsbruck, Innsbruck, Austria.
BMC Anesthesiol. 2021 May 12;21(1):145. doi: 10.1186/s12871-021-01365-y.
Flow-controlled ventilation (FCV) is a novel ventilation method increasingly being used clinically, particularly during the current COVID-19 pandemic. However, the continuous flow pattern in FCV during inspiration and expiration has a significant impact on respiratory parameters and ventilatory settings compared to conventional ventilation modes. In addition, the constant flow combined with direct intratracheal pressure measurement allows determination of dynamic compliance and ventilation settings can be adjusted accordingly, reflecting a personalized ventilation approach.
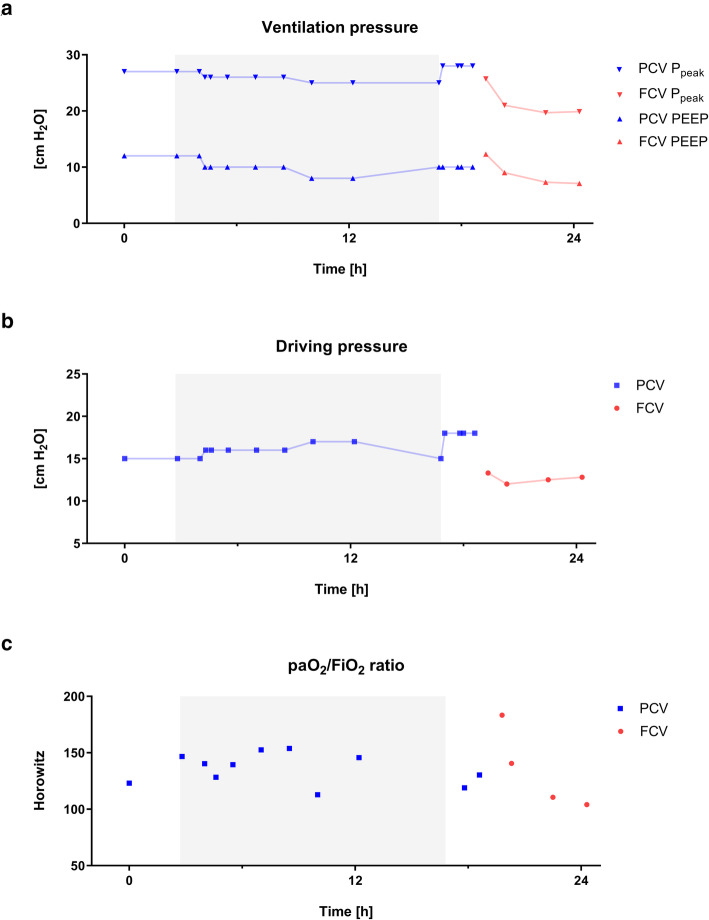
A 50-year old women with confirmed SARS-CoV-2 infection suffering from acute respiratory distress syndrome (ARDS) was admitted to a tertiary medical center. Initial ventilation occurred with best standard of care pressure-controlled ventilation (PCV) and was then switched to FCV, by adopting PCV ventilator settings. This led to an increase in oxygenation by 30 %. Subsequently, to reduce invasiveness of mechanical ventilation, FCV was individualized by dynamic compliance guided adjustment of both, positive end-expiratory pressure and peak pressure; this intervention reduced driving pressure from 18 to 12 cm HO. However, after several hours, compliance further deteriorated which resulted in a tidal volume of only 4.7 ml/kg.
An individualized FCV approach increased oxygenation parameters in a patient suffering from severe COVID-19 related ARDS. Direct intratracheal pressure measurements allow for determination of dynamic compliance and thus optimization of ventilator settings, thereby reducing applied and dissipated energy. However, although desirable, this personalized ventilation strategy may reach its limits when lung function is so severely impaired that patient's oxygenation has to be ensured at the expense of lung protective ventilation concepts.
流量控制通气(FCV)是一种临床上越来越常用的新型通气方法,尤其是在当前的新冠疫情期间。然而,与传统通气模式相比,FCV在吸气和呼气过程中的持续气流模式对呼吸参数和通气设置有显著影响。此外,恒定气流与直接气管内压力测量相结合,可以测定动态顺应性,并据此调整通气设置,体现了个性化通气方法。
一名确诊感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)且患有急性呼吸窘迫综合征(ARDS)的50岁女性被收治入一家三级医疗中心。最初采用最佳标准的压力控制通气(PCV)进行通气,随后通过采用PCV通气设置切换至FCV。这使氧合增加了30%。随后,为降低机械通气的侵入性,通过动态顺应性指导调整呼气末正压和峰值压力,对FCV进行个体化;该干预使驱动压力从18 cm H₂O降至12 cm H₂O。然而,数小时后,顺应性进一步恶化,导致潮气量仅为4.7 ml/kg。
个体化的FCV方法提高了一名患有严重新冠相关ARDS患者的氧合参数。直接气管内压力测量可测定动态顺应性,从而优化通气设置,进而减少施加和耗散的能量。然而,尽管这种个性化通气策略很理想,但当肺功能严重受损以至于必须以牺牲肺保护性通气理念为代价来确保患者氧合时,该策略可能会达到其极限。