Department of Viroscience, Postgraduate School of Molecular Medicine, Erasmus MC, Rotterdam, the Netherlands.
Center for Vaccine Research, School of Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania, USA.
mSphere. 2021 May 12;6(3):e00237-21. doi: 10.1128/mSphere.00237-21.
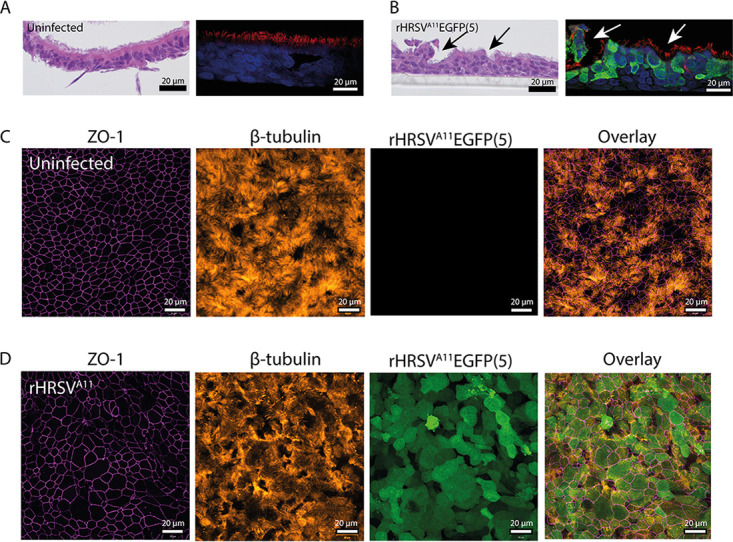
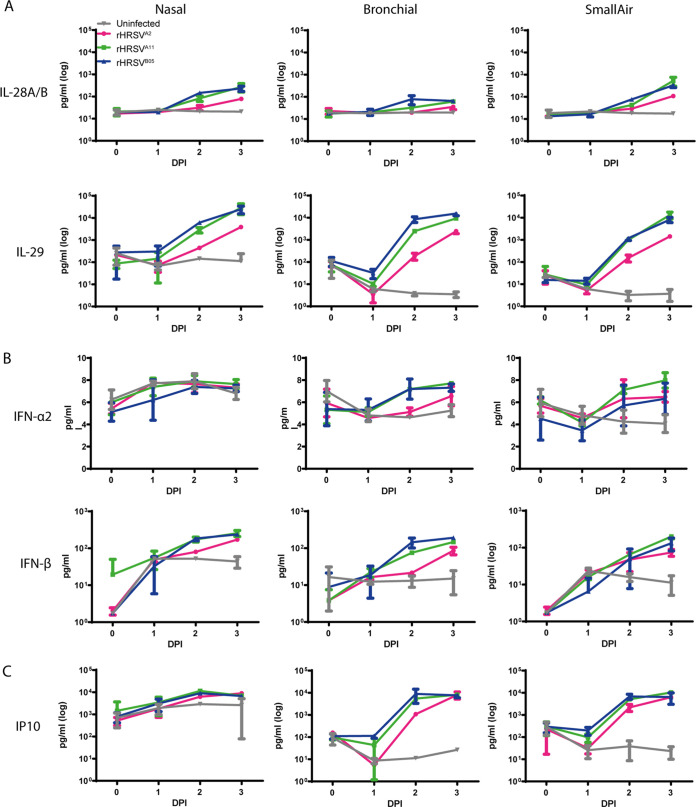
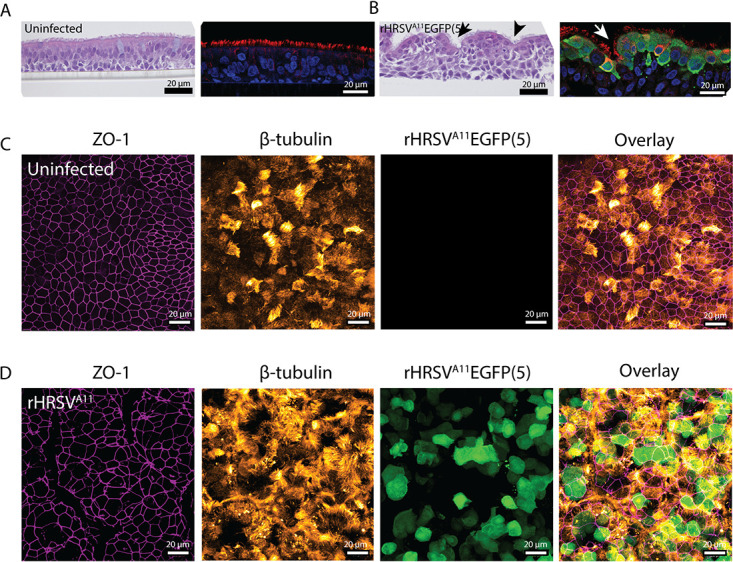
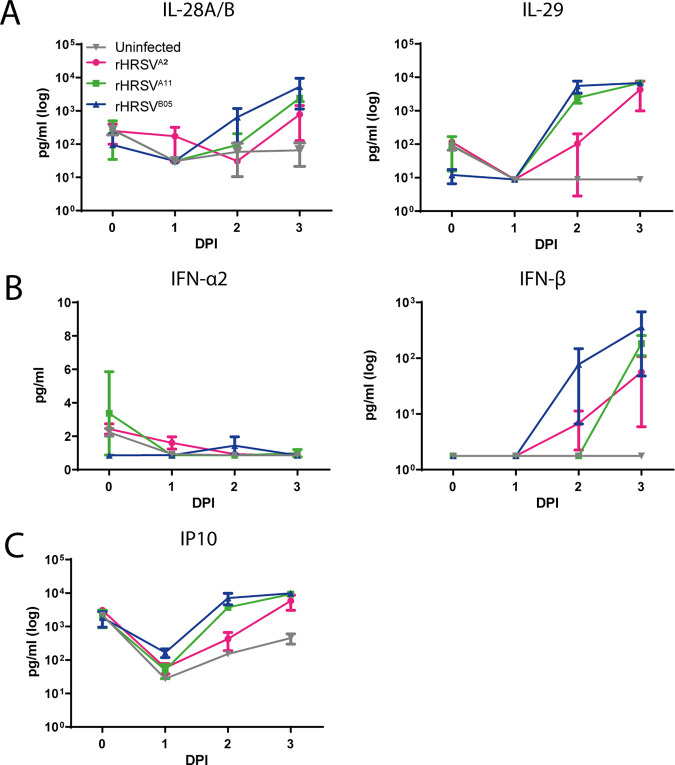
Human respiratory syncytial virus (HRSV) is the leading cause of bronchiolitis in infants. Two subgroups of HRSV (A and B) routinely cocirculate. Most research has been performed with HRSV-A strains because these are easier to culture than HRSV-B strains. In this study, we aimed to compare the replicative fitness and HRSV-induced innate cytokine responses of HRSV-A and HRSV-B strains in disease-relevant cell culture models. We used two recombinant (r) clinical isolate-based HRSV strains (A11 and B05) and one recombinant laboratory-adapted HRSV strain (A2) to infect commercially available nasal, bronchial, and small-airway cultures. Epithelial cells from all anatomical locations were susceptible to HRSV infection despite the induction of a dominant type III interferon response. Subgroup A viruses disseminated and replicated faster than the subgroup B virus. Additionally, we studied HRSV infection and innate responses in airway organoids (AOs) cultured at air-liquid interface (ALI). Results were similar to the commercially obtained bronchial cells. In summary, we show that HRSV replicates well in cells from both the upper and the lower airways, with a slight replicative advantage for subgroup A viruses. Lastly, we showed that AOs cultured at ALI are a valuable model for studying HRSV and that they can be used in the future to study factors that influence HRSV disease severity. Human respiratory syncytial virus (HRSV) is the major cause of bronchiolitis and pneumonia in young infants and causes almost 200,000 deaths per year. Currently, there is no vaccine or treatment available, only a prophylactic monoclonal antibody (palivizumab). An important question in HRSV pathogenesis research is why only a fraction (1 to 3%) of infants develop severe disease. Model systems comprising disease-relevant HRSV isolates and accurate and reproducible cell culture models are indispensable to study infection, replication, and innate immune responses. Here, we used differentiated AOs cultured at ALI to model the human airways. Subgroup A viruses replicated better than subgroup B viruses, which we speculate fits with epidemiological findings that subgroup A viruses cause more severe disease in infants. By using AOs cultured at ALI, we present a highly relevant, robust, and reproducible model that allows for future studies into what drives severe HRSV disease.
人类呼吸道合胞病毒(HRSV)是婴儿细支气管炎的主要病因。HRSV 有两个亚群(A 和 B),通常同时存在。大多数研究都是针对 HRSV-A 株进行的,因为这些株比 HRSV-B 株更容易培养。在这项研究中,我们旨在比较 HRSV-A 和 HRSV-B 株在相关疾病细胞培养模型中的复制适应性和 HRSV 诱导的先天细胞因子反应。我们使用了两种重组(r)临床分离株(A11 和 B05)和一种重组实验室适应株(A2)感染商业上可获得的鼻腔、支气管和小气道培养物。尽管诱导了主要的 III 型干扰素反应,但所有解剖部位的上皮细胞都容易受到 HRSV 感染。亚组 A 病毒的传播和复制速度比亚组 B 病毒快。此外,我们还在空气-液体界面(ALI)培养的气道类器官(AO)中研究了 HRSV 感染和先天反应。结果与商业获得的支气管细胞相似。总之,我们表明 HRSV 可以很好地复制上呼吸道和下呼吸道的细胞,亚组 A 病毒具有轻微的复制优势。最后,我们表明,在 ALI 培养的 AO 是研究 HRSV 的有价值的模型,并且将来可以用于研究影响 HRSV 疾病严重程度的因素。人类呼吸道合胞病毒(HRSV)是婴幼儿细支气管炎和肺炎的主要病因,每年导致近 20 万人死亡。目前,尚无疫苗或治疗方法,只有一种预防性单克隆抗体(帕利珠单抗)。HRSV 发病机制研究中的一个重要问题是为什么只有一小部分(1%至 3%)婴儿会出现严重疾病。包含相关 HRSV 分离株的模型系统和准确且可重复的细胞培养模型对于研究感染、复制和先天免疫反应是必不可少的。在这里,我们使用在 ALI 培养的分化的 AO 来模拟人类气道。亚组 A 病毒的复制能力优于亚组 B 病毒,我们推测这与流行病学发现相符,即亚组 A 病毒在婴儿中引起更严重的疾病。通过使用在 ALI 培养的 AO,我们提出了一种高度相关、稳健且可重复的模型,允许对导致严重 HRSV 疾病的原因进行未来研究。