Center for Cancer and Immunology Research, Children's Research Institute, Children's National Hospital, Washington, DC, USA.
National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD, USA.
J Clin Immunol. 2021 Aug;41(6):1146-1153. doi: 10.1007/s10875-021-01046-y. Epub 2021 May 13.
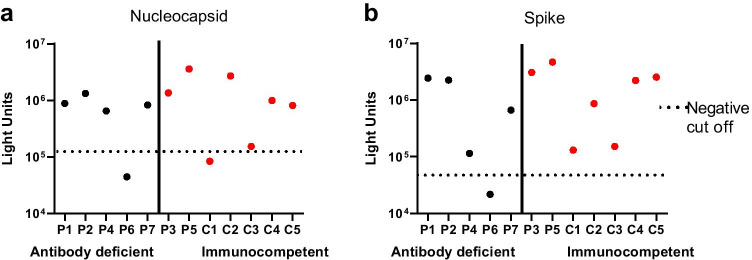
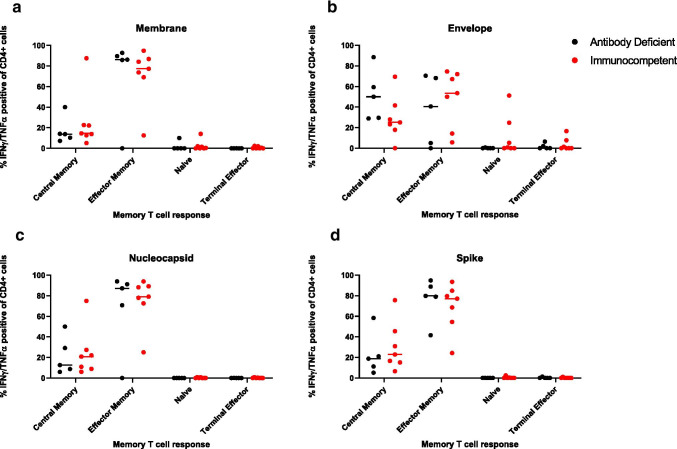
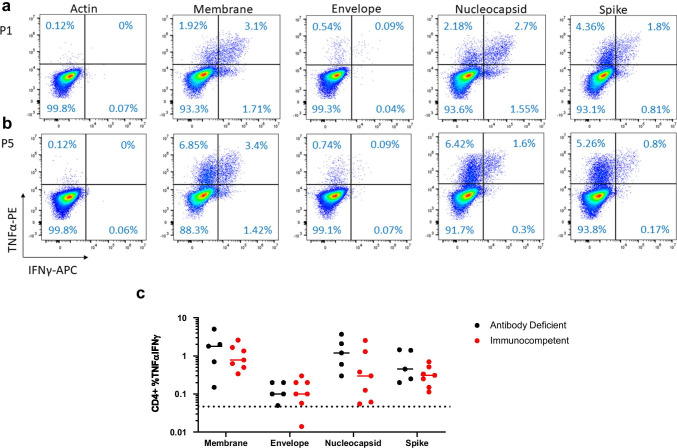
Immunocompromised patients, including those with inborn errors of immunity (IEI), may be at increased risk for severe or prolonged infections with SARS-CoV-2 (Zhu et al. N Engl J Med. 382:727-33, 2020; Guan et al. 2020; Minotti et al. J Infect. 81:e61-6, 2020). While antibody and T cell responses to SARS-CoV-2 structural proteins are well described in healthy convalescent donors, adaptive humoral and cellular immunity has not yet been characterized in patients with antibody deficiency (Grifoni et al. Cell. 181:1489-1501 e1415, 2020; Burbelo et al. 2020; Long et al. Nat Med. 26:845-8, 2020; Braun et al. 2020). Herein, we describe the clinical course, antibody, and T cell responses to SARS-CoV-2 structural proteins in a cohort of adult and pediatric patients with antibody deficiencies (n = 5) and controls (related and unrelated) infected with SARS-CoV-2. Five patients within the same family (3 with antibody deficiency, 2 immunocompetent controls) showed antibody responses to nucleocapsid and spike proteins, as well as SARS-CoV-2 specific T cell immunity at days 65-84 from onset of symptoms. No significant difference was identified between immunocompromised patients and controls. Two additional unrelated, adult patients with common variable immune deficiency were assessed. One did not show antibody response, but both demonstrated SARS-CoV-2-specific T cell immunity when evaluated 33 and 76 days, respectively, following SARS-CoV-2 diagnosis. This report is the first to show robust T cell activity and humoral immunity against SARS-CoV-2 structural proteins in some patients with antibody deficiency. Given the reliance on spike protein in most candidate vaccines (Folegatti et al. Lancet. 396:467-78, 2020; Jackson et al. N Engl J Med. 383:1920-31, 2020), the responses are encouraging. Additional studies will be needed to further define the timing of onset of immunity, longevity of the immune response, and variability of response in immunocompromised patients.
免疫功能低下的患者,包括患有先天性免疫缺陷的患者(IEI),可能面临严重或持续感染 SARS-CoV-2 的风险增加(Zhu 等人,N Engl J Med. 382:727-33, 2020;Guan 等人,2020;Minotti 等人,J Infect. 81:e61-6, 2020)。尽管在健康的恢复期供体中已经很好地描述了针对 SARS-CoV-2 结构蛋白的抗体和 T 细胞反应,但针对抗体缺陷患者的适应性体液和细胞免疫尚未得到描述(Grifoni 等人,Cell. 181:1489-1501 e1415, 2020;Burbelo 等人,2020;Long 等人,Nat Med. 26:845-8, 2020;Braun 等人,2020)。在此,我们描述了一组患有抗体缺陷(n = 5)和对照(相关和无关)的成年和儿科患者对 SARS-CoV-2 结构蛋白的临床病程、抗体和 T 细胞反应。来自同一家庭的 5 名患者(3 名患有抗体缺陷,2 名免疫功能正常的对照)在症状发作后 65-84 天显示出针对核衣壳和刺突蛋白的抗体反应,以及 SARS-CoV-2 特异性 T 细胞免疫。在免疫功能低下的患者和对照组之间未发现显著差异。另外评估了 2 名患有常见可变免疫缺陷的无关成年患者。其中 1 名患者未显示抗体反应,但当分别在 SARS-CoV-2 诊断后 33 天和 76 天时评估时,2 名患者均显示出 SARS-CoV-2 特异性 T 细胞免疫。这是首次在一些抗体缺陷患者中显示出针对 SARS-CoV-2 结构蛋白的强大 T 细胞活性和体液免疫的报告。鉴于大多数候选疫苗都依赖于刺突蛋白(Folegatti 等人,Lancet. 396:467-78, 2020;Jackson 等人,N Engl J Med. 383:1920-31, 2020),这些反应令人鼓舞。需要进一步的研究来进一步确定免疫的起始时间、免疫反应的持续时间以及免疫功能低下患者的反应变异性。