Department of Intensive Care, Amsterdam UMC, Amsterdam, Noord-Holland, The Netherlands.
Institute for Cardiovascular Research (ICaR-VU), Amsterdam UMC, Amsterdam, Noord-Holland, The Netherlands.
PLoS One. 2021 May 13;16(5):e0250740. doi: 10.1371/journal.pone.0250740. eCollection 2021.
In the context of an ongoing debate on the potential risks of hypoxemia and hyperoxemia, it seems prudent to maintain the partial arterial oxygen pressure (PaO2) in a physiological range during administration of supplemental oxygen. The PaO2 and peripheral oxygen saturation (SpO2) are closely related and both are used to monitor oxygenation status. However, SpO2 values cannot be used as an exact substitute for PaO2. The aim of this study in acutely ill and stable patients was to determine at which SpO2 level PaO2 is more or less certain to be in the physiological range.
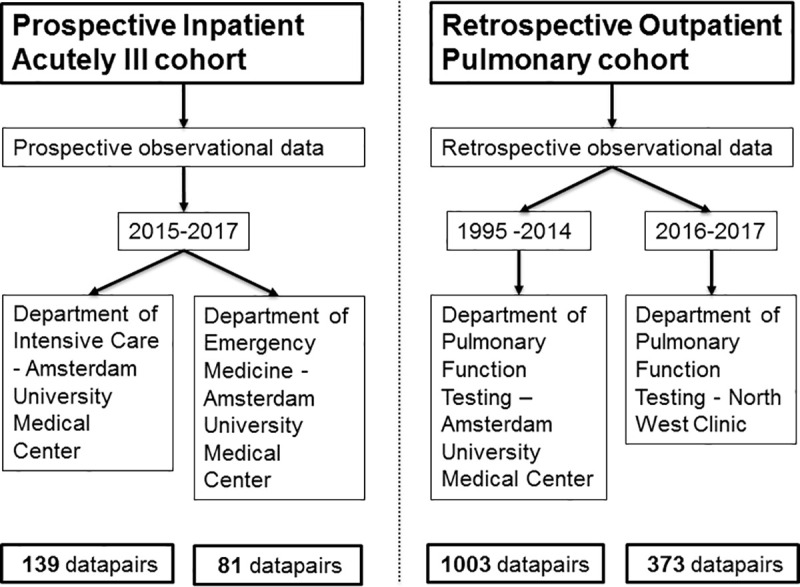
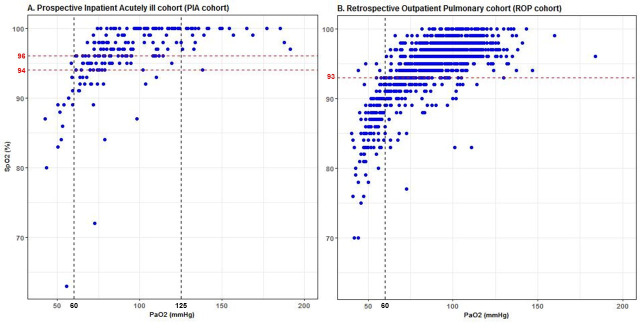
This is an observational study prospectively collecting data pairs of PaO2 and SpO2 values in patients admitted to the emergency room or intensive care unit (Prospective Inpatient Acutely ill cohort; PIA cohort). A second cohort of retrospective data of patients who underwent pulmonary function testing was also included (Retrospective Outpatient Pulmonary cohort; ROP cohort). Arterial hypoxemia was defined as PaO2 < 60 mmHg and hyperoxemia as PaO2 > 125 mmHg. The SpO2 cut-off values with the lowest risk of hypoxemia and hyperoxemia were determined as the 95th percentile of the observed SpO2 values corresponding with the observed hypoxemic and hyperoxemic PaO2 values.
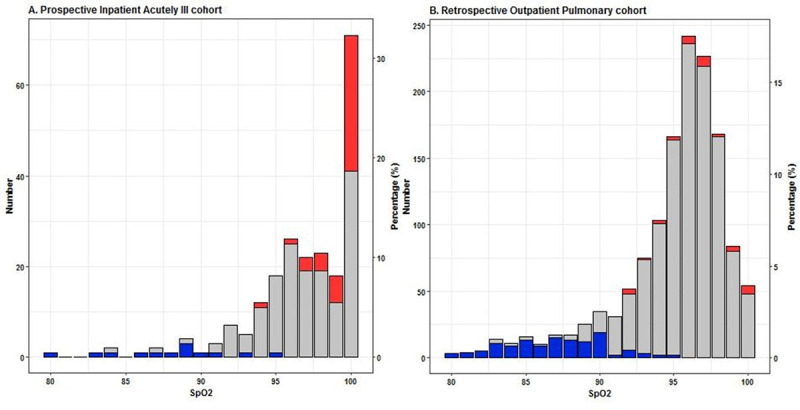
220 data pairs were collected in the PIA cohort. 95% of hypoxemic PaO2 measurements occurred in patients with an SpO2 below 94%, and 95% of hyperoxemic PaO2 measurements occurred in patients with an SpO2 above 96%. Additionally in the 1379 data pairs of the ROP cohort, 95% of hypoxemic PaO2 measurements occurred in patients with an SpO2 below 93%.
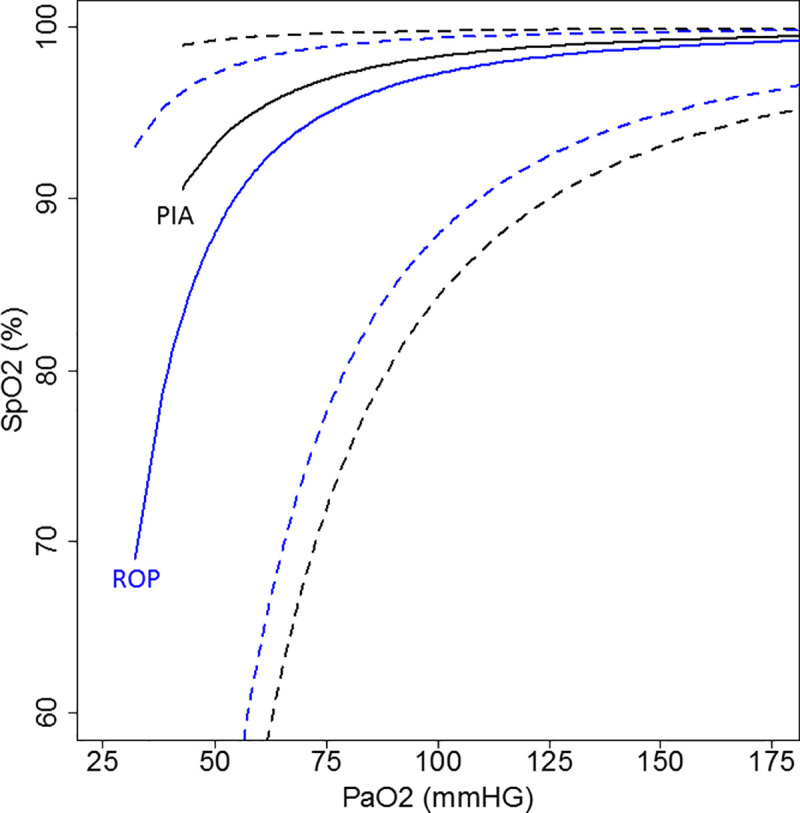
The SpO2 level marking an increased risk of arterial hypoxemia is not substantially different in acutely ill versus stable patients. In acutely ill patients receiving supplemental oxygen an SpO2 target of 95% maximizes the likelihood of maintaining PaO2 in the physiological range.
在持续争论低氧血症和高氧血症潜在风险的背景下,在给予补充氧气时将部分动脉血氧分压(PaO2)维持在生理范围内似乎是谨慎的。PaO2 和外周血氧饱和度(SpO2)密切相关,两者都用于监测氧合状态。然而,SpO2 值不能作为 PaO2 的准确替代值。本研究旨在急性和稳定患者中确定 SpO2 水平达到多少时 PaO2 更有可能处于生理范围内。
这是一项前瞻性收集急诊或重症监护病房(急性住院患者前瞻性队列;PIA 队列)患者 PaO2 和 SpO2 值数据对的观察性研究。还纳入了接受肺功能测试的回顾性数据患者的第二队列(回顾性门诊肺队列;ROP 队列)。动脉低氧血症定义为 PaO2 < 60 mmHg,高氧血症定义为 PaO2 > 125 mmHg。确定最低风险低氧血症和高氧血症的 SpO2 截断值为与观察到的低氧血症和高氧血症 PaO2 值相对应的观察到的 SpO2 值的第 95 个百分位数。
PIA 队列共收集了 220 对数据。95%的低氧血症 PaO2 测量发生在 SpO2 低于 94%的患者中,95%的高氧血症 PaO2 测量发生在 SpO2 高于 96%的患者中。此外,ROP 队列的 1379 对数据中,95%的低氧血症 PaO2 测量发生在 SpO2 低于 93%的患者中。
在急性和稳定患者中,SpO2 水平标记动脉低氧血症风险增加的程度没有显著差异。在接受补充氧气的急性患者中,SpO2 目标为 95%可最大程度地提高维持 PaO2 在生理范围内的可能性。