de Jager Justine, Brouwer Fleur, Reijman Jeroen, van der Palen Roel L F, Steggerda Sylke J, Visser Remco, Te Pas Arjan B, Dekker Janneke
Division of Neonatology, Department of Pediatrics, Leiden University Medical Center, Leiden, The Netherlands.
Division of Pediatric Cardiology, Department of Pediatrics, Leiden University Medical Center, Leiden, The Netherlands.
Eur J Pediatr. 2024 May;183(5):2455-2461. doi: 10.1007/s00431-024-05506-6. Epub 2024 Mar 12.
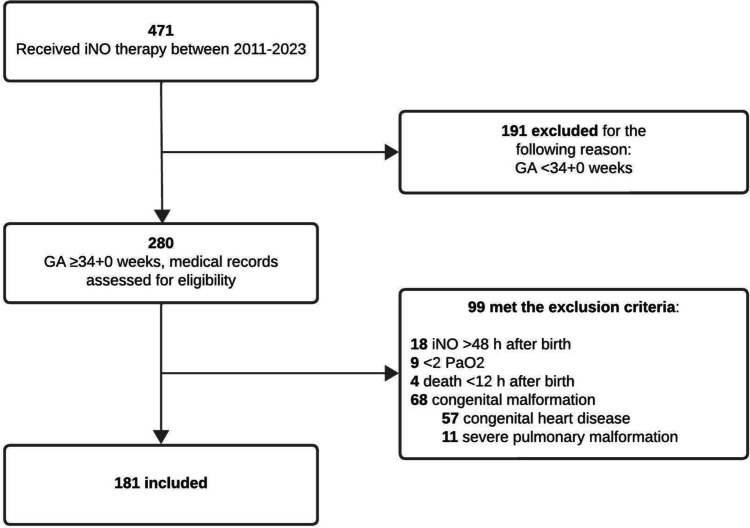
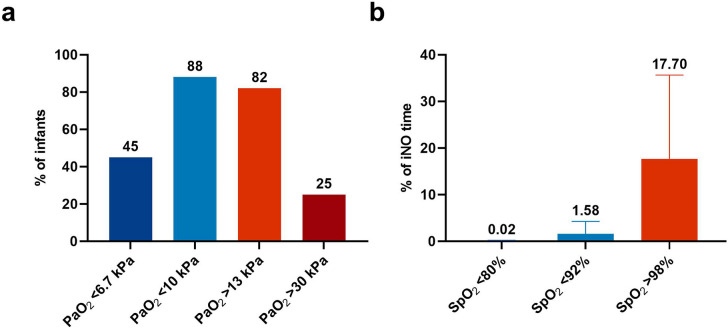
High concentrations of oxygen are often needed to optimize oxygenation in infants with persistent pulmonary hypertension (PPHN), but this can also increase the risk of hyperoxemia. We determined the occurrence of hyperoxemia in infants treated for PPHN. Medical records of infants ≥ 34 + 0 weeks gestational age (GA) who received inhaled nitric oxide (iNO) were retrospectively reviewed for oxygenation parameters during iNO therapy. Oxygen was manually titrated to target arterial oxygen tension (PaO) 10-13 kPa and peripheral oxygen saturation (SpO) 92-98%. The main study outcomes were the incidence and duration of hyperoxemia and hypoxemia and the fraction of inspired oxygen (FiO). A total of 181 infants were included. The median FiO was 0.43 (IQR 0.34-0.56) and the maximum FiO was 1.0 in 156/181 (86%) infants, resulting in at least one PaO > 13 kPa in 149/181 (82%) infants, of which 46/149 (31%) infants had minimal one PaO > 30 kPa. SpO was > 98% in 179/181 (99%) infants for 17.7% (8.2-35.6%) of the iNO time. PaO < 10 kPa occurred in 160/181 (88%) infants, of which 81/160 (51%) infants had minimal one PaO < 6.7 kPa. SpO was < 92% in 169/181 (93%) infants for 1.6% (0.5-4.3%) of the iNO time. Conclusion: While treatment of PPHN is focused on preventing and reversing hypoxemia, hyperoxemia occurs inadvertently in most patients. What is Known: • High concentrations of oxygen are often needed to prevent hypoxemia-induced deterioration of PPHN, but this can also increase the risk of hyperoxemia. • Infants with persistent pulmonary hypertension may be particularly vulnerable to the toxic effects of oxygen, and hyperoxemia could further induce pulmonary vasoconstriction, potentially worsening the condition. What is New: • Hyperoxemia occurs in the majority of infants with PPHN during treatment with iNO. • Infants with PPHN spent a considerably longer period with saturations above the target range compared to saturations below the target range.
对于患有持续性肺动脉高压(PPHN)的婴儿,通常需要高浓度氧气来优化氧合,但这也会增加高氧血症的风险。我们确定了接受PPHN治疗的婴儿中高氧血症的发生率。对孕周≥34+0周且接受吸入一氧化氮(iNO)治疗的婴儿的病历进行回顾性分析,以获取iNO治疗期间的氧合参数。手动调节氧气以使动脉血氧分压(PaO)目标值为10 - 13kPa,外周血氧饱和度(SpO)目标值为92 - 98%。主要研究结果包括高氧血症和低氧血症的发生率、持续时间以及吸入氧分数(FiO)。共纳入181名婴儿。FiO的中位数为0.43(四分位间距0.34 - 0.56),181名婴儿中有156名(86%)的最大FiO为1.0,这导致181名婴儿中有149名(82%)至少有一次PaO>13kPa,其中149名婴儿中有46名(31%)至少有一次PaO>30kPa。181名婴儿中有179名(99%)的SpO在iNO治疗时间的17.7%(8.2 - 35.6%)内>98%。181名婴儿中有160名(88%)出现PaO<10kPa,其中160名婴儿中有81名(51%)至少有一次PaO<6.7kPa。181名婴儿中有169名(93%)的SpO在iNO治疗时间的1.6%(0.5 - 4.3%)内<92%。结论:虽然PPHN的治疗重点是预防和纠正低氧血症,但大多数患者会无意中出现高氧血症。已知信息:• 通常需要高浓度氧气来预防低氧血症导致的PPHN病情恶化,但这也会增加高氧血症的风险。• 患有持续性肺动脉高压的婴儿可能对氧气的毒性作用特别敏感,高氧血症可能会进一步诱发肺血管收缩,从而可能使病情恶化。新发现:• 在iNO治疗期间,大多数PPHN婴儿会出现高氧血症。• 与饱和度低于目标范围相比,PPHN婴儿饱和度高于目标范围的时间要长得多。