Department of Respiratory Therapy, College of Medicine, Chang Gung University, Taoyuan, 33353, Taiwan.
Division of Pulmonary and Critical Care Medicine, Chang Gung Memorial Hospital, 5, Fu-Hsin St. Gweishan, Taoyuan, 33353, Taiwan.
Sci Rep. 2021 May 13;11(1):10186. doi: 10.1038/s41598-021-89463-2.
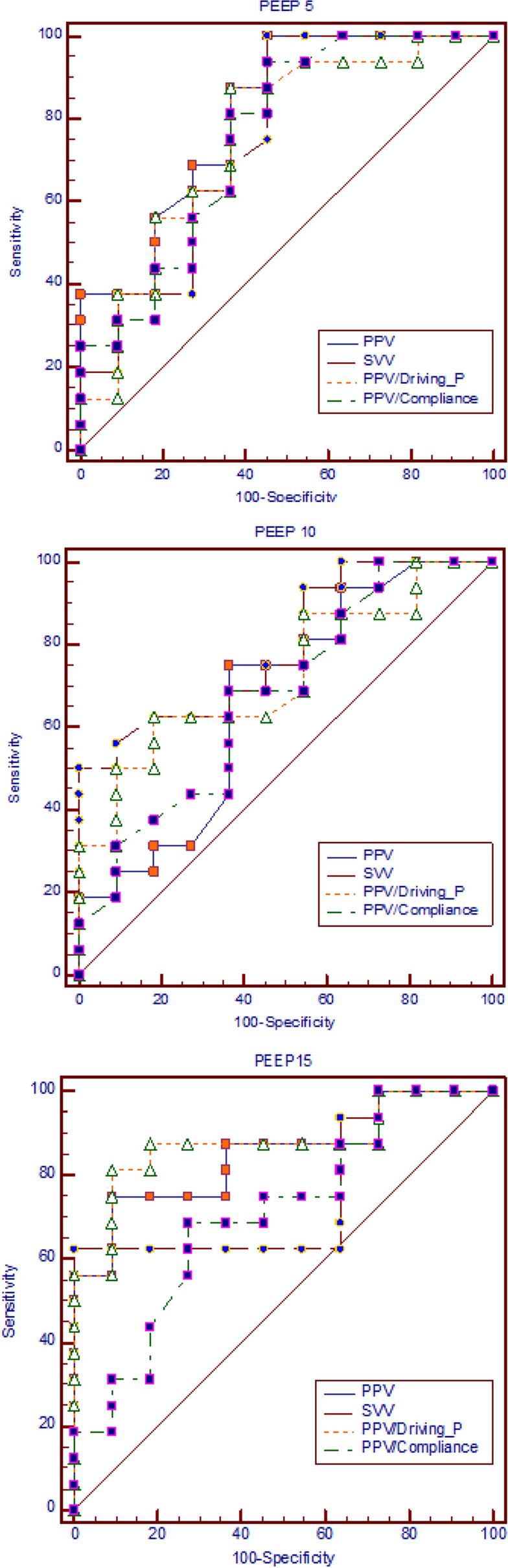
The prediction accuracy of pulse pressure variation (PPV) for fluid responsiveness was suggested to be unreliable in low tidal volume (VT) ventilation. However, high PEEP can cause ARDS patients relatively hypovolemic and more fluid responsive. We hypothesized that high PEEP 15 cmHO can offset the disadvantage of low VT and improve the predictive performance of PPV. We prospectively enrolled 27 hypovolemic ARDS patients ventilated with low VT 6 ml/kg and three levels of PEEP (5, 10, 15 cmHO) randomly. Each stage lasted for at least 5 min to allow for equilibration of hemodynamics and pulmonary mechanics. Then, fluid expansion was given with 500 ml hydroxyethyl starch (Voluven 130/70). The hemodynamics and PPV were automatically measured with a PiCCO2 monitor. The PPV values were significantly higher during PEEP15 than those during PEEP5 and PEEP10. PPV during PEEP15 precisely predicts fluid responsiveness with a cutoff value 8.8% and AUC (area under the ROC curve) of ROC (receiver operating characteristic curve) 0.847, higher than the AUC during PEEP5 (0.81) and PEEP10 (0.668). Normalizing PPV with driving pressure (PPV/Driving-P) increased the AUC of PPV to 0.875 during PEEP15. In conclusions, high PEEP 15 cmHO can counteract the drawback of low VT and preserve the predicting accuracy of PPV in ARDS patients.
脉压变异度(PPV)对液体反应性的预测准确性在小潮气量(VT)通气时被认为不可靠。然而,高水平呼气末正压通气(PEEP)可能导致 ARDS 患者相对低血容量和更具液体反应性。我们假设高水平 PEEP(15cmH2O)可以抵消小潮气量的不利影响,提高 PPV 的预测性能。我们前瞻性地招募了 27 例低血容量性 ARDS 患者,随机接受小潮气量(6ml/kg)和三种不同水平的 PEEP(5、10、15cmH2O)通气。每个阶段至少持续 5 分钟,以允许血流动力学和肺力学达到平衡。然后,给予 500ml 羟乙基淀粉(万汶 130/70)进行液体扩张。使用脉搏指示连续心排血量监测仪自动测量血流动力学和 PPV。PEEP15 时的 PPV 值明显高于 PEEP5 和 PEEP10 时的 PPV 值。PEEP15 时的 PPV 能够准确预测液体反应性,截断值为 8.8%,ROC 曲线下面积(AUC)为 0.847,高于 PEEP5(0.81)和 PEEP10(0.668)时的 AUC。用驱动压(PPV/Driving-P)校正后,PPV 的 AUC 在 PEEP15 时增加到 0.875。总之,高水平 PEEP(15cmH2O)可以抵消小潮气量的缺点,并维持 ARDS 患者中 PPV 的预测准确性。