Service de réanimation médicale et maladies infectieuses, Hôpital Bichat- Claude Bernard, Assistance Publique des Hôpitaux de Paris, 18 rue Henri Huchard, F-75018 Paris, France.
Crit Care. 2011;15(2):R85. doi: 10.1186/cc10083. Epub 2011 Mar 7.
Fluid responsiveness prediction is of utmost interest during acute respiratory distress syndrome (ARDS), but the performance of respiratory pulse pressure variation (ΔRESPPP) has scarcely been reported. In patients with ARDS, the pathophysiology of ΔRESPPP may differ from that of healthy lungs because of low tidal volume (Vt), high respiratory rate, decreased lung and sometimes chest wall compliance, which increase alveolar and/or pleural pressure. We aimed to assess ΔRESPPP in a large ARDS population.
Our study population of nonarrhythmic ARDS patients without inspiratory effort were considered responders if their cardiac output increased by >10% after 500-ml volume expansion.
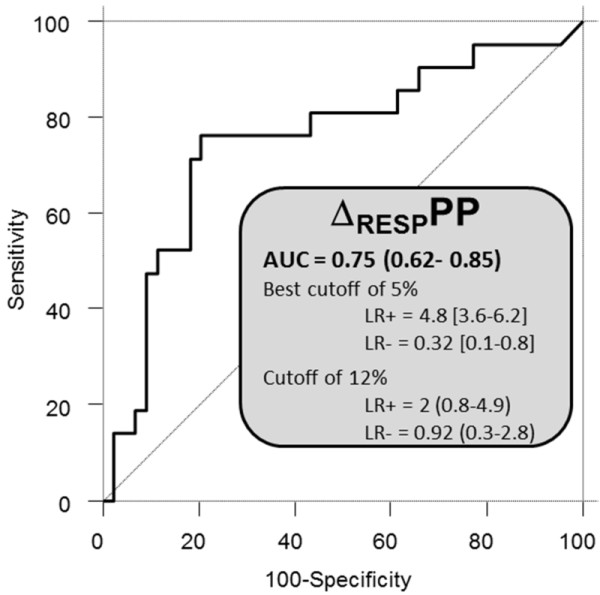
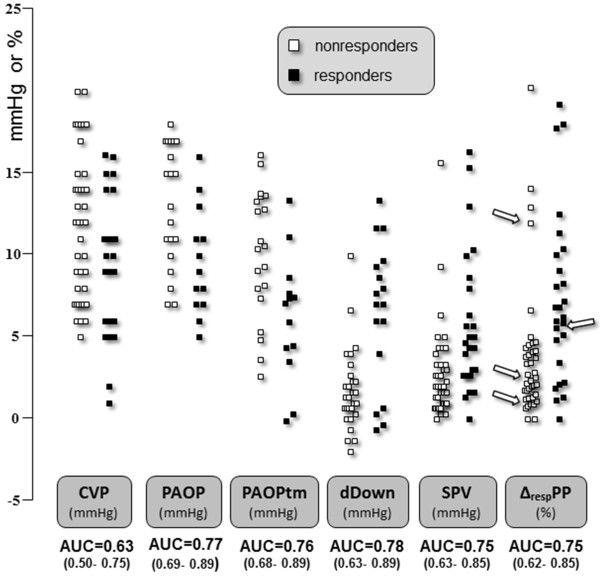
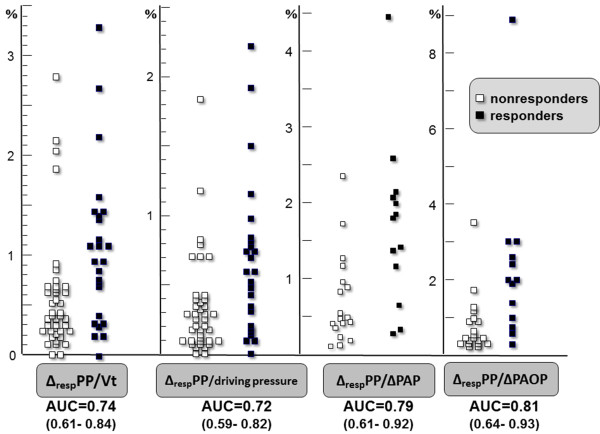
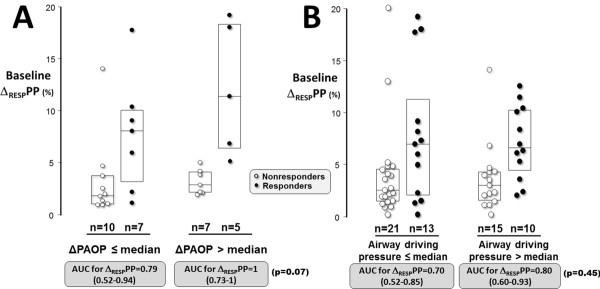
Among the 65 included patients (26 responders), the area under the receiver-operating curve (AUC) for ΔRESPPP was 0.75 (95% confidence interval (CI95): 0.62 to 0.85), and a best cutoff of 5% yielded positive and negative likelihood ratios of 4.8 (CI95: 3.6 to 6.2) and 0.32 (CI95: 0.1 to 0.8), respectively. Adjusting ΔRESPPP for Vt, airway driving pressure or respiratory variations in pulmonary artery occlusion pressure (ΔPAOP), a surrogate for pleural pressure variations, in 33 Swan-Ganz catheter carriers did not markedly improve its predictive performance. In patients with ΔPAOP above its median value (4 mmHg), AUC for ΔRESPPP was 1 (CI95: 0.73 to 1) as compared with 0.79 (CI95: 0.52 to 0.94) otherwise (P = 0.07). A 300-ml volume expansion induced a ≥ 2 mmHg increase of central venous pressure, suggesting a change in cardiac preload, in 40 patients, but none of the 28 of 40 nonresponders responded to an additional 200-ml volume expansion.
During protective mechanical ventilation for early ARDS, partly because of insufficient changes in pleural pressure, ΔRESPPP performance was poor. Careful fluid challenges may be a safe alternative.
在急性呼吸窘迫综合征(ARDS)期间,液体反应性预测至关重要,但呼吸脉冲压变化(ΔRESPPP)的性能鲜有报道。在 ARDS 患者中,由于潮气量(Vt)低、呼吸频率高、肺顺应性和/或胸壁顺应性降低,导致肺泡和/或胸膜压力增加,因此 ΔRESPPP 的病理生理学可能与健康肺不同。我们旨在评估 ARDS 大人群中的 ΔRESPPP。
我们的非心律失常 ARDS 患者研究人群,如果其心输出量在 500ml 容量扩张后增加>10%,则被认为是有反应者。
在 65 名纳入患者(26 名有反应者)中,ΔRESPPP 的受试者工作特征曲线下面积(AUC)为 0.75(95%置信区间(CI95):0.62 至 0.85),最佳截断值为 5%,阳性和阴性似然比分别为 4.8(CI95:3.6 至 6.2)和 0.32(CI95:0.1 至 0.8)。在 33 名 Swan-Ganz 导管携带者中,根据 Vt、气道驱动压或肺动脉闭塞压(ΔPAOP)的呼吸变化(ΔPAOP 的替代指标)调整 ΔRESPPP,并未显著改善其预测性能。在 ΔPAOP 高于中位数(4mmHg)的患者中,ΔRESPPP 的 AUC 为 1(CI95:0.73 至 1),而在其他患者中为 0.79(CI95:0.52 至 0.94)(P=0.07)。在 40 名患者中,300ml 容量扩张引起中心静脉压升高≥2mmHg,提示心脏前负荷发生变化,但在 40 名无反应者中的 28 名无反应者对另外 200ml 容量扩张无反应。
在 ARDS 早期进行保护性机械通气时,由于胸膜压力变化不足,ΔRESPPP 的性能较差。谨慎的液体挑战可能是一种安全的替代方法。