Haematology Department, Fiona Stanley Hospital, Perth, WA, Australia.
Division of Hematology, Department of Internal Medicine, Mayo Clinic, Rochester, MN, USA.
Blood Cancer J. 2021 May 15;11(5):90. doi: 10.1038/s41408-021-00483-7.
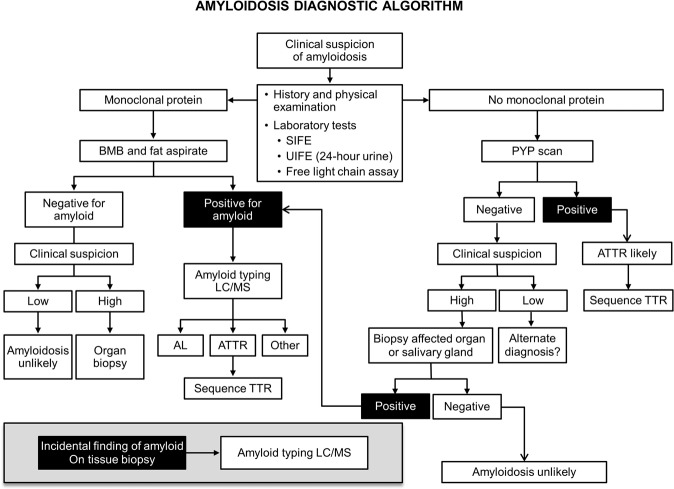
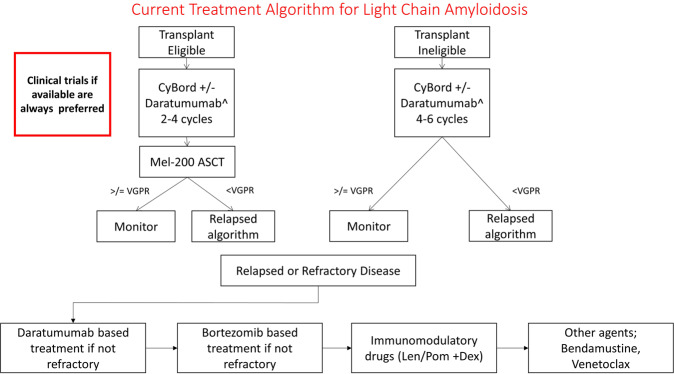
Immunoglobulin light chain amyloidosis (AL) commonly presents with nephrotic range proteinuria, heart failure with preserved ejection fraction, nondiabetic peripheral neuropathy, unexplained hepatomegaly or diarrhea, and should be considered in patients presenting with these symptoms. More importantly, patients being monitored for smoldering multiple myeloma and a monoclonal gammopathy of undetermined significance (MGUS) are at risk for developing AL amyloidosis. MGUS and myeloma patients that have atypical features, including unexplained weight loss; lower extremity edema, early satiety, and dyspnea on exertion should be considered at risk for light chain amyloidosis. Overlooking the diagnosis of light chain amyloidosis leading to therapy delay is common, and it represents an error of diagnostic consideration. Herein we provide a review of established and investigational treatments for patients with AL amyloidosis and provide algorithms for workup and management of these patients.
免疫球蛋白轻链淀粉样变性(AL)常表现为肾病范围蛋白尿、射血分数保留的心力衰竭、非糖尿病性周围神经病、不明原因的肝肿大或腹泻,出现这些症状时应考虑该病。更重要的是,正在监测冒烟型多发性骨髓瘤和意义未明的单克隆丙种球蛋白病(MGUS)的患者有发生 AL 淀粉样变性的风险。MGUS 和骨髓瘤患者有不典型特征,包括不明原因的体重减轻;下肢水肿、早饱和活动时呼吸困难,应认为有发生轻链淀粉样变性的风险。漏诊轻链淀粉样变性导致治疗延迟很常见,这是诊断考虑的失误。本文综述了 AL 淀粉样变性患者的既定和研究性治疗方法,并提供了这些患者的检查和管理算法。