Go Ellen, van Veenendaal Mira, Manlhiot Cedric, Schneider Rayfel, McCrindle Brian W, Yeung Rae S M
The Hospital for Sick Children, Division of Rheumatology, University of Toronto, Toronto, ON, Canada.
University Medical Center Utrecht, Division of Rheumatology, Wilhelmina Children's Hospital, Utrecht, Netherlands.
Front Pediatr. 2021 Apr 28;9:665815. doi: 10.3389/fped.2021.665815. eCollection 2021.
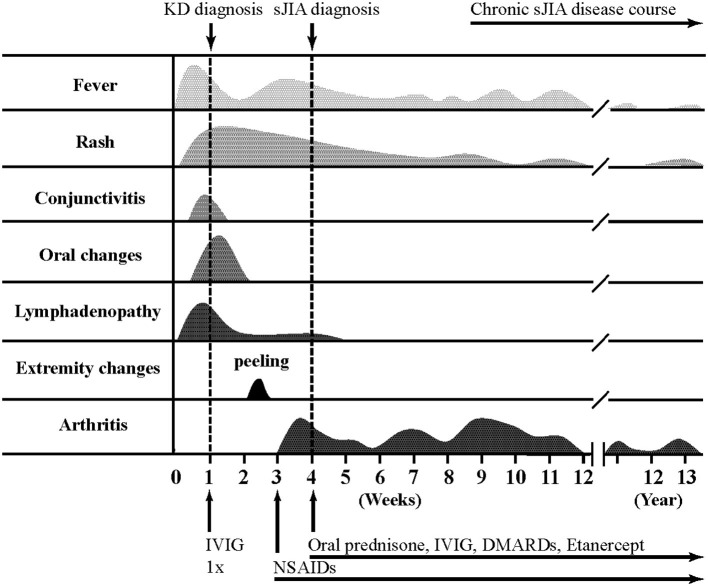
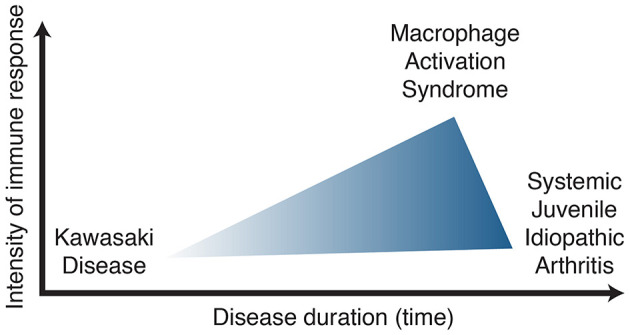
Kawasaki disease (KD) and systemic juvenile idiopathic arthritis (sJIA) are two distinct systemic inflammatory diseases of childhood. Each diagnosis is based on criteria, but numerous clinical features are overlapping. As no specific diagnostic tests are available, differentiation between both disease entities can be challenging. Here, we describe the disease course of patients with co-diagnosis of both KD and sJIA (KD/sJIA). All our KD ( = 1765) and sJIA ( = 112) cases were critically reviewed for co-diagnosis of KD/sJIA. Eight KD/sJIA cases were identified and their clinical presentation, treatment regimens, coronary artery outcome and complications are herein described. Each KD/sJIA patient fulfilled diagnostic criteria for KD and for sJIA. Ongoing fever, rash and arthritis were present in each patient. The KD/sJIA patients had recalcitrant KD requiring multiple doses of intravenous immunoglobulin and steroids. Five patients had coronary artery dilatation at KD diagnosis, which resolved in all by 6 weeks. Pericardial effusion was present in 5 patients. One KD/sJIA patient developed macrophage activation syndrome. In conclusion, a small proportion (0.5%) of our KD patients evolved into sJIA, and 7% of our sJIA population presented initially as KD. KD/sJIA patients were characterized by a recalcitrant KD course and a high prevalence of coronary artery dilatation. Patients with co-diagnoses may provide a clue to potentially shared immunopathology in KD and sJIA, leading us to posit that both entities may be part of the same clinical spectrum.
川崎病(KD)和全身型幼年特发性关节炎(sJIA)是儿童期两种不同的全身性炎症性疾病。每种疾病的诊断都基于相应标准,但众多临床特征存在重叠。由于没有可用的特异性诊断测试,区分这两种疾病实体可能具有挑战性。在此,我们描述了同时诊断为KD和sJIA(KD/sJIA)的患者的疾病进程。我们对所有KD(n = 1765)和sJIA(n = 112)病例进行了严格审查,以确定是否存在KD/sJIA的共诊断情况。共识别出8例KD/sJIA病例,并在此描述了他们的临床表现、治疗方案、冠状动脉结局及并发症。每例KD/sJIA患者均符合KD和sJIA的诊断标准。每位患者均存在持续发热、皮疹和关节炎。KD/sJIA患者的KD病情顽固,需要多次静脉注射免疫球蛋白和使用类固醇。5例患者在KD诊断时出现冠状动脉扩张,所有患者在6周时均缓解。5例患者出现心包积液。1例KD/sJIA患者发生巨噬细胞活化综合征。总之,我们的KD患者中有一小部分(0.5%)演变为sJIA,而我们的sJIA患者中有7%最初表现为KD。KD/sJIA患者的特点是KD病程顽固且冠状动脉扩张的患病率高。共诊断的患者可能为KD和sJIA潜在的共同免疫病理学提供线索,使我们推测这两种疾病可能属于同一临床谱系的一部分。