Kohsaka Shun, Okami Suguru, Kanda Eiichiro, Kashihara Naoki, Yajima Toshitaka
Department of Cardiology, Keio University School of Medicine, Tokyo, Japan.
Cardiovascular, Renal, and Metabolism, Medical Affairs, AstraZeneca KK, Osaka, Japan.
Mayo Clin Proc Innov Qual Outcomes. 2021 Jan 19;5(2):274-285. doi: 10.1016/j.mayocpiqo.2020.10.001. eCollection 2021 Apr.
To examine the association between hyperkalemia and long-term cardiovascular and renal outcomes in patients with chronic kidney disease.
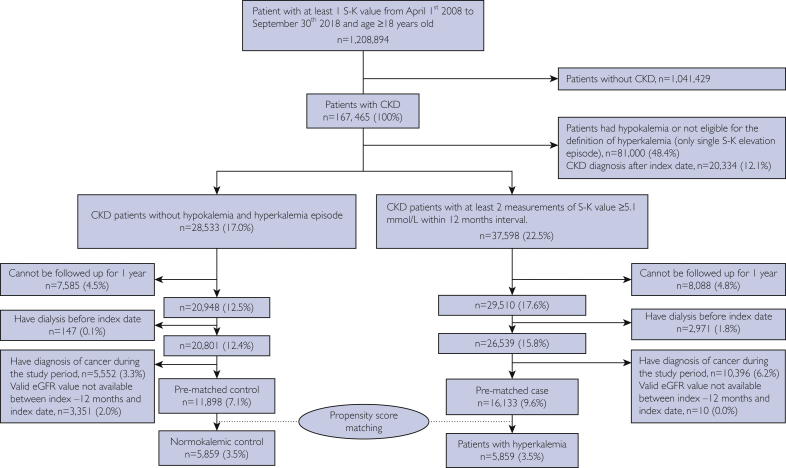
An observational retrospective cohort study was performed using a Japanese hospital claims registry, Medical Data Vision (April 1, 2008, to September 30, 2018). Of 1,208,894 patients with at least 1 potassium measurement, 167,465 patients with chronic kidney disease were selected based on codes or estimated glomerular filtration rate (eGFR) less than 60 mL/min/1.73 m. Hyperkalemia was defined as at least 2 potassium measurements of 5.1 mmol/L or greater within 12 months. Normokalemic controls were patients without a record of potassium levels of 5.1 mmol/L or greater and 3.5 mmol/L or less. Changes in eGFRs and hazard ratios of death, hospitalization for cardiac events, heart failure, and renal replacement therapy introduction were assessed between propensity score-matched hyperkalemic patients and normokalemic controls.
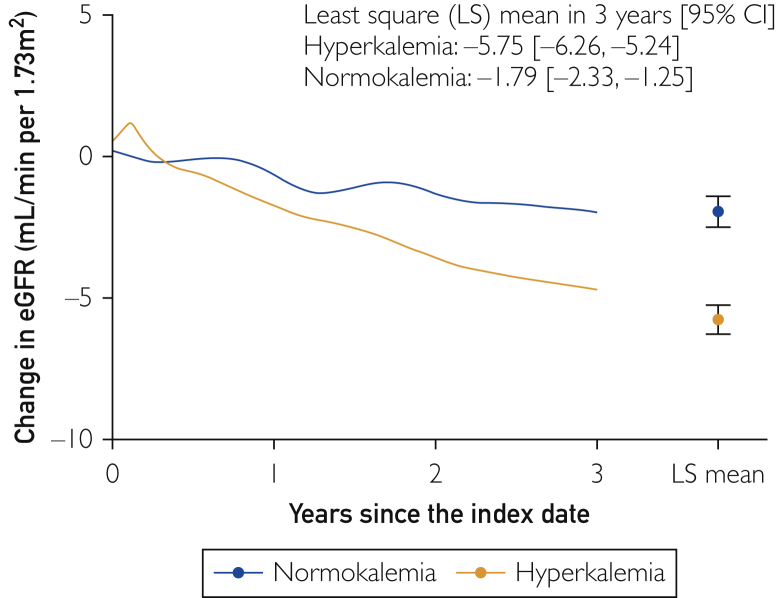
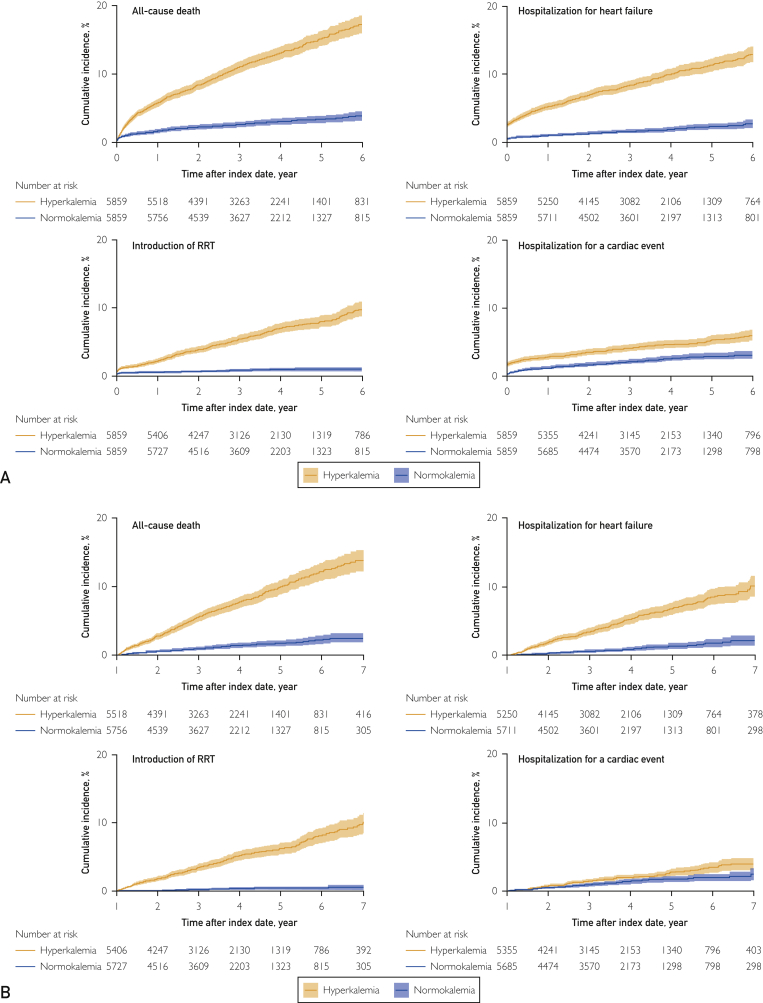
Of 16,133 hyperkalemic patients and 11,898 normokalemic controls eligible for analyses, 5859 (36.3%) patients and 5859 (49.2%) controls were selected after propensity score matching. The mean follow-up period was 3.5 years. The 3-year eGFR change in patients and controls was -5.75 and -1.79 mL/min/1.73 m, respectively. Overall, hyperkalemic patients had higher risks for death, hospitalization for cardiac events, heart failure, and renal replacement therapy introduction than controls, with hazard ratios of 4.40 (95% CI, 3.74 to 5.18), 1.95 (95% CI, 1.59 to 2.39), 5.09 (95% CI, 4.17 to 6.21), and 7.54 (95% CI, 5.73 to 9.91), respectively.
Hyperkalemia was associated with significant risks for mortality and adverse clinical outcomes, with more rapid decline of renal function. These findings underscore the significance of hyperkalemia as a predisposition to future adverse events in patients with chronic kidney disease.
研究慢性肾脏病患者高钾血症与长期心血管及肾脏预后之间的关联。
利用日本医院理赔登记系统“医学数据视界”(2008年4月1日至2018年9月30日)进行了一项观察性回顾性队列研究。在1,208,894例至少进行过1次血钾测量的患者中,根据编码或估算肾小球滤过率(eGFR)低于60 mL/min/1.73 m²,选取了167,465例慢性肾脏病患者。高钾血症定义为在12个月内至少有2次血钾测量值达到或高于5.1 mmol/L。血钾正常的对照者为无血钾水平达到或高于5.1 mmol/L且低于或等于3.5 mmol/L记录的患者。在倾向得分匹配的高钾血症患者和血钾正常的对照者之间,评估了eGFR的变化以及死亡、心脏事件住院、心力衰竭和开始肾脏替代治疗的风险比。
在16,133例符合分析条件的高钾血症患者和11,898例血钾正常的对照者中,经过倾向得分匹配后,分别选取了5859例(36.3%)患者和5859例(49.2%)对照者。平均随访期为3.5年。患者和对照者3年的eGFR变化分别为-5.75和-1.79 mL/min/1.73 m²。总体而言,高钾血症患者死亡、心脏事件住院、心力衰竭和开始肾脏替代治疗的风险高于对照者,风险比分别为4.40(95%CI,3.74至5.18)、1.95(95%CI,1.59至2.39)、5.09(95%CI,4.17至6.21)和7.54(95%CI,5.73至9.91)。
高钾血症与死亡及不良临床结局的显著风险相关,且肾功能下降更快。这些发现强调了高钾血症作为慢性肾脏病患者未来不良事件易患因素的重要性。