Division of Cardiovascular Medicine, Amagasaki-Chuo Hospital, 1-12-1 Shioe, Amagasaki, Hyogo, 661-0976, Japan.
Department of Medical Informatics, Osaka University Graduate School of Medicine, Suita, Japan.
ESC Heart Fail. 2021 Aug;8(4):3145-3155. doi: 10.1002/ehf2.13420. Epub 2021 May 16.
The prognostic importance of admission systolic blood pressure (SBP) in heart failure with preserved ejection fraction (HFpEF) is elusive. We aimed to clarify the pathophysiological differences between patients categorized with admission SBP among HFpEF patients.
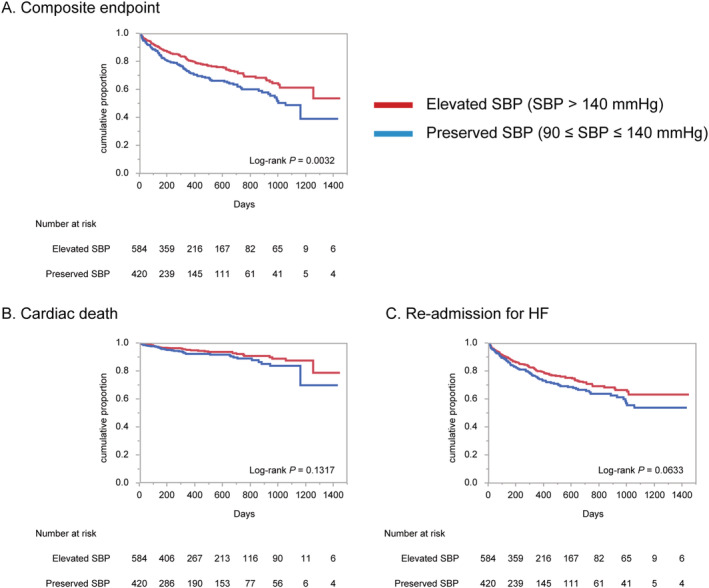
We studied 1008 inpatients from PURSUIT-HFpEF, a multicentre prospective observational registry. We classified patients as having elevated (>140 mmHg), preserved (90-140 mmHg), or low (<90 mmHg) admission SBP. Most cases had elevated (n = 584) or preserved (n = 420) SBP; the four cases with low SBP were excluded. Univariable Cox regression testing revealed that preserved SBP patients had a higher risk of a composite of cardiac death and heart failure re-hospitalization [hazard ratio (HR) 1.48, 95% confidence interval (CI) 1.14-1.92, P = 0.0035] than elevated SBP patients. In multivariable Cox regression models, while prior heart failure hospitalization (HR 1.36, 95% CI 1.01-2.84, P = 0.0453), atrial fibrillation (HR 1.82, 95% CI 1.10-2.99, P = 0.0209), and N-terminal pro-B-type natriuretic peptide (HR 1.94, 95% CI 1.10-3.43, P = 0.0229) at discharge were significantly associated with adverse outcomes in elevated SBP patients, N-terminal pro-B-type natriuretic peptide (HR 2.06, 95% CI 1.04-4.07, P = 0.0373) and right ventricular-pulmonary artery uncoupling reflected by the tricuspid annular plane systolic excursion/pulmonary artery systolic pressure ratio (HR 0.19, 95% CI 0.05-0.65, P = 0.0075) at discharge were significant prognostic factors in preserved SBP patients.
Patients with preserved admission SBP had significant higher risks for adverse outcomes than those with elevated SBP in HFpEF. Tricuspid annular plane systolic excursion/pulmonary artery systolic pressure was the distinctive prognostic factor between the two groups.
射血分数保留的心衰(HFpEF)患者入院时收缩压(SBP)的预后意义尚不清楚。本研究旨在明确 HFpEF 患者中根据入院 SBP 分类的患者之间的病理生理学差异。
我们研究了来自 PURSUIT-HFpEF 的 1008 名住院患者,这是一项多中心前瞻性观察性研究。我们将患者分为入院时 SBP 升高(>140mmHg)、保留(90-140mmHg)或降低(<90mmHg)。大多数患者的 SBP 升高(n=584)或保留(n=420);4 例 SBP 降低的患者被排除在外。单变量 Cox 回归检验显示,与 SBP 升高的患者相比,SBP 保留的患者发生心脏死亡和心力衰竭再住院的复合终点的风险更高[风险比(HR)1.48,95%置信区间(CI)1.14-1.92,P=0.0035]。在多变量 Cox 回归模型中,虽然既往心力衰竭住院(HR 1.36,95%CI 1.01-2.84,P=0.0453)、心房颤动(HR 1.82,95%CI 1.10-2.99,P=0.0209)和出院时的 N 末端 B 型利钠肽前体(HR 1.94,95%CI 1.10-3.43,P=0.0229)与 SBP 升高患者的不良结局显著相关,但出院时的 N 末端 B 型利钠肽前体(HR 2.06,95%CI 1.04-4.07,P=0.0373)和三尖瓣环平面收缩期位移/肺动脉收缩压比值(HR 0.19,95%CI 0.05-0.65,P=0.0075)反映的右心室-肺动脉解耦与 SBP 保留患者的预后显著相关。
HFpEF 患者中,与 SBP 升高的患者相比,SBP 保留的患者发生不良结局的风险显著更高。三尖瓣环平面收缩期位移/肺动脉收缩压比值是两组之间的独特预后因素。