Department of Internal Medicine Yale School of Medicine New Haven CT.
Department of Internal Medicine Bridgeport HospitalYale-New Haven Health System Bridgeport CT.
J Am Heart Assoc. 2021 Jul 6;10(13):e021084. doi: 10.1161/JAHA.121.021084. Epub 2021 May 15.
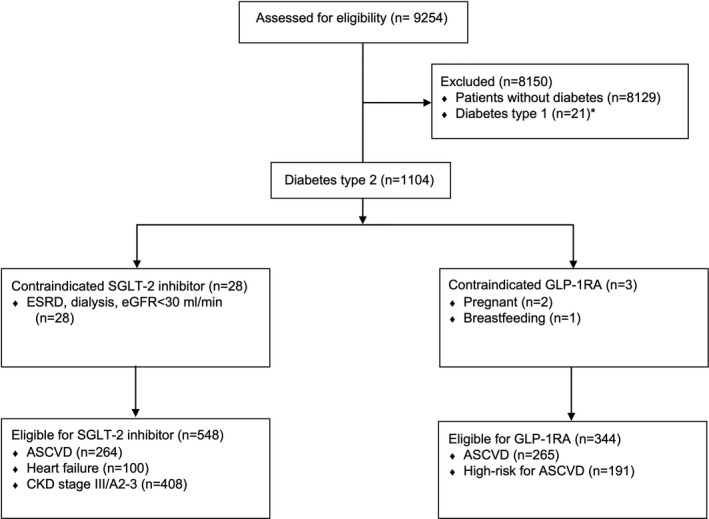
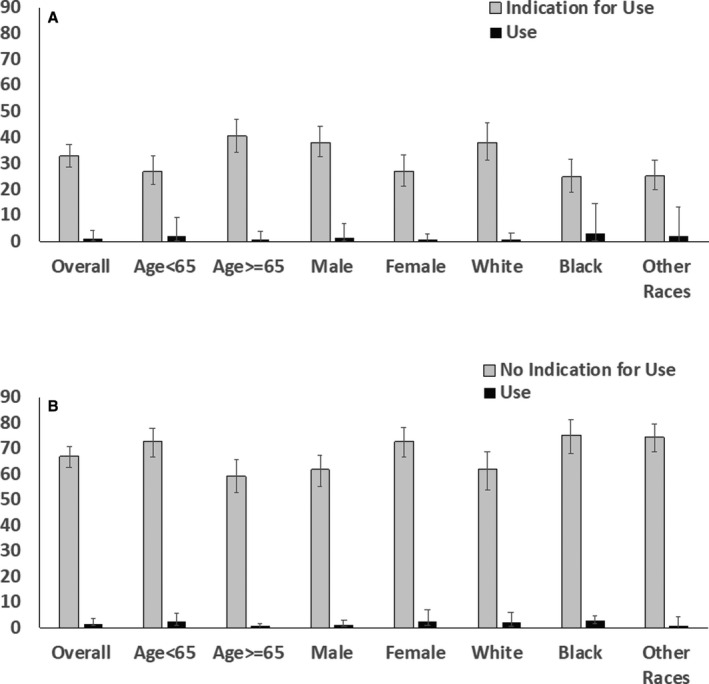
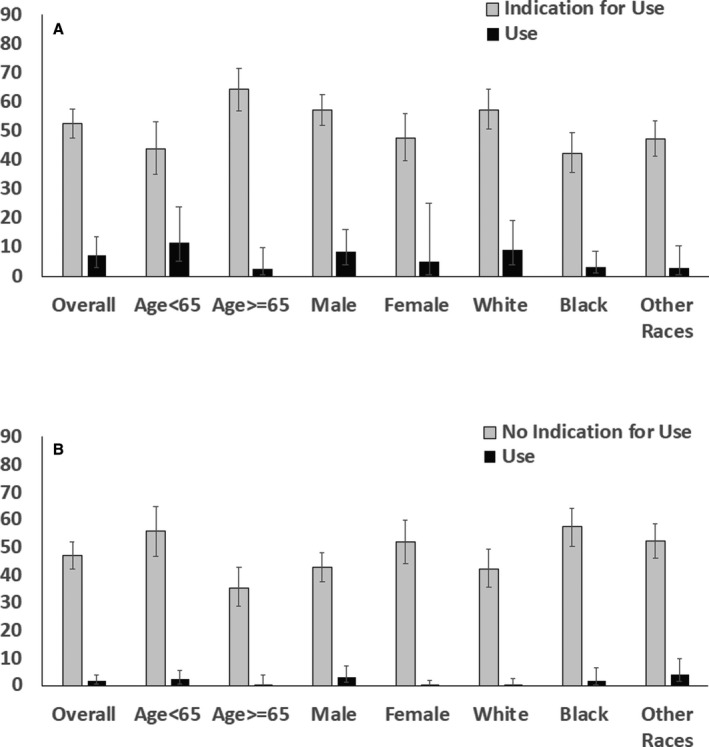
Background SGLT-2 (sodium glucose transporter-2) inhibitors and GLP-1RAs (glucagon-like peptide-1 receptor agonists) effectively lowered cardiovascular risk in large clinical trials for patients with type 2 diabetes mellitus at high risk for these complications, and have been recommended by guidelines. To evaluate the contemporary landscape in which these recommendations would be implemented, we examined the use of these medications according to clinical guideline practice. Methods and Results In the National Health and Nutrition Examination Survey for 2017 to 2018, we defined compelling indications for SGLT-2 inhibitors by the presence of atherosclerotic cardiovascular disease, heart failure, or chronic kidney disease, and for GLP-1RAs by the presence of established or high-risk atherosclerotic cardiovascular disease, based on large clinical trials that have been incorporated in guideline recommendations of the American College of Cardiology and American Diabetes Association. We then evaluated use of these medications among patients with physician-diagnosed type 2 diabetes mellitus. All analyses incorporated complex survey design to produce nationally representative estimates. A total 1104 of 9254 sampled individuals had type 2 diabetes mellitus, representing 10.6% (95% CI, 9.7%-11.6%) of the US population or 33.2 million adults nationally. Of these, 52.6% (95% CI, 47.7%-57.5%) had an indication for SGLT-2 inhibitors, 32.8% (95% CI, 28.8%-37.2%) for GLP-1RAs, and 26.6% (95% CI, 22.2%-31.7%) for both medications. During 2017 to 2018, 4.5% (95% CI, 2.4%-8.2%) were treated with SGLT-2 inhibitors and 1.5% (95% CI, 0.7%-3.2%) with GLP-1RAs. Atherosclerotic cardiovascular disease, heart failure, or chronic kidney disease were not independently associated with SGLT-2 inhibitor or GLP-1RA use in patients with diabetes mellitus. Conclusions Despite a large number of patients being eligible for guideline-recommended cardiorenal protective therapies, there are substantial gaps in the use of SGLT-2 inhibitors and GLP-1RAs, limiting their public health benefits.
钠-葡萄糖协同转运蛋白 2(SGLT-2)抑制剂和胰高血糖素样肽-1 受体激动剂(GLP-1RA)在大型临床试验中有效地降低了 2 型糖尿病高危患者的心血管风险,并且已经被指南推荐。为了评估这些推荐在当代的实施情况,我们根据临床指南实践检查了这些药物的使用情况。
在 2017 年至 2018 年的全国健康与营养调查中,我们根据已被纳入美国心脏病学会和美国糖尿病协会指南推荐的大型临床试验,将动脉粥样硬化性心血管疾病、心力衰竭或慢性肾脏病定义为 SGLT-2 抑制剂的明确适应证,将已确诊或高危动脉粥样硬化性心血管疾病定义为 GLP-1RA 的明确适应证。然后,我们评估了这些药物在有医生诊断的 2 型糖尿病患者中的使用情况。所有分析都采用复杂的调查设计,以产生具有全国代表性的估计值。在抽样的 9254 人中,有 1104 人患有 2 型糖尿病,占美国人口的 10.6%(95%CI,9.7%-11.6%)或全国 3320 万成年人的 10.6%。其中,52.6%(95%CI,47.7%-57.5%)有 SGLT-2 抑制剂适应证,32.8%(95%CI,28.8%-37.2%)有 GLP-1RA 适应证,26.6%(95%CI,22.2%-31.7%)有两种药物的适应证。在 2017 年至 2018 年期间,有 4.5%(95%CI,2.4%-8.2%)的患者接受 SGLT-2 抑制剂治疗,1.5%(95%CI,0.7%-3.2%)的患者接受 GLP-1RA 治疗。在患有糖尿病的患者中,动脉粥样硬化性心血管疾病、心力衰竭或慢性肾脏病与 SGLT-2 抑制剂或 GLP-1RA 的使用均无独立相关性。
尽管有大量患者符合指南推荐的心脏肾脏保护治疗标准,但 SGLT-2 抑制剂和 GLP-1RA 的使用仍存在很大差距,限制了它们的公共卫生效益。