Department of Rheumatology and Inflammation Research, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg.
Department of Medicine, Rheumatology Unit, Center for Molecular Medicine, Karolinska Institute, Karolinska University Hospital, Stockholm, Sweden.
Rheumatology (Oxford). 2022 Mar 2;61(3):1233-1242. doi: 10.1093/rheumatology/keab454.
Treatment with CTLA-4Ig blocks T-cell activation and is clinically effective in RA. However, it is unknown if specific CD4+ T-cell subsets in blood at baseline predict remission after CTLA-4Ig, or other biological treatments with different modes of action, and how treatment affects CD4+ T cells in patients with untreated early RA (eRA).
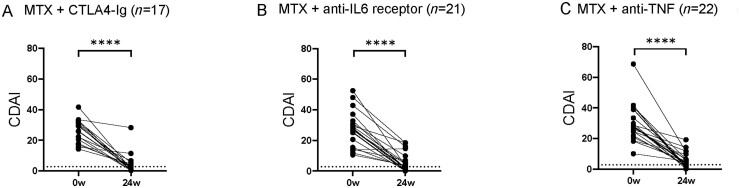
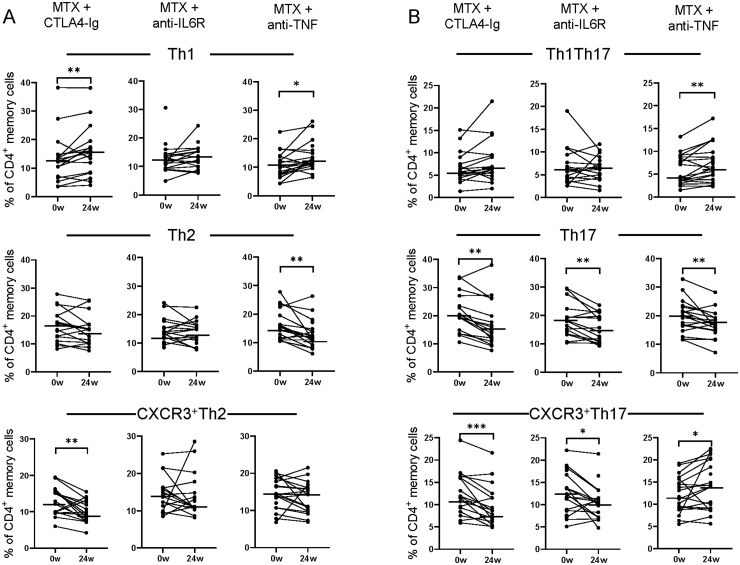
This study included 60 patients with untreated eRA from a larger randomized trial. They were treated with methotrexate combined with CTLA-4Ig (abatacept, n = 17), anti-IL6 receptor (tocilizumab, n = 21) or anti-TNF (certolizumab-pegol, n = 22). Disease activity was assessed by clinical disease activity index (CDAI), DAS28, swollen joint counts, tender joint counts, CRP and ESR. The primary outcome was CDAI remission (CDAI ≤ 2.8) at week 24. Proportions of 12 CD4+ T-cell subsets were measured by flow cytometry at baseline and after 4, 12 and 24 weeks of treatment.
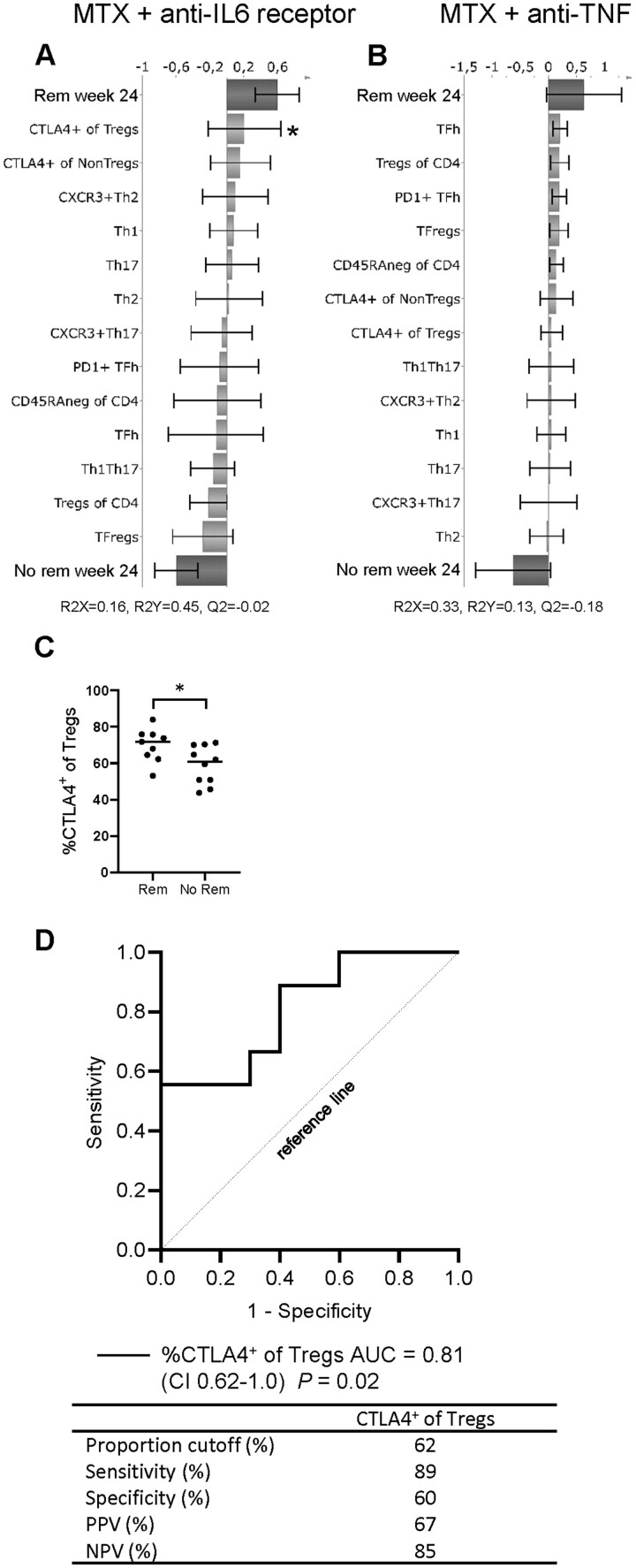
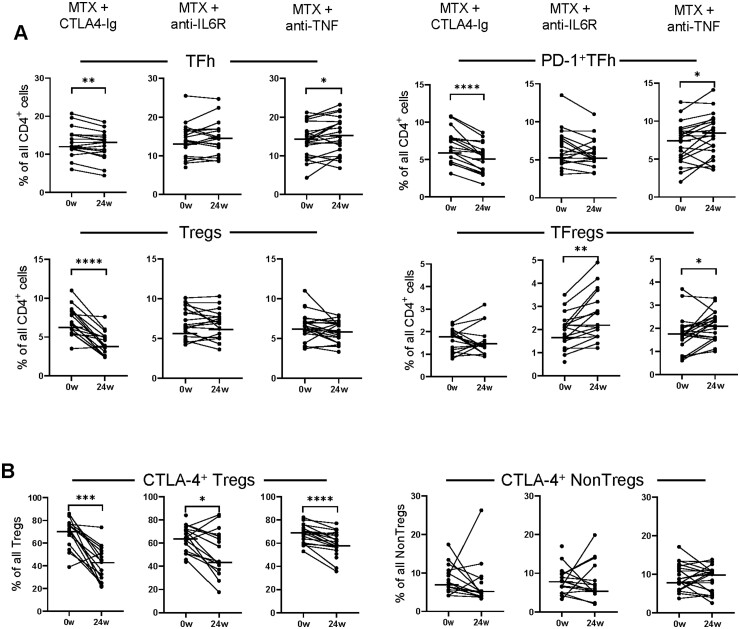
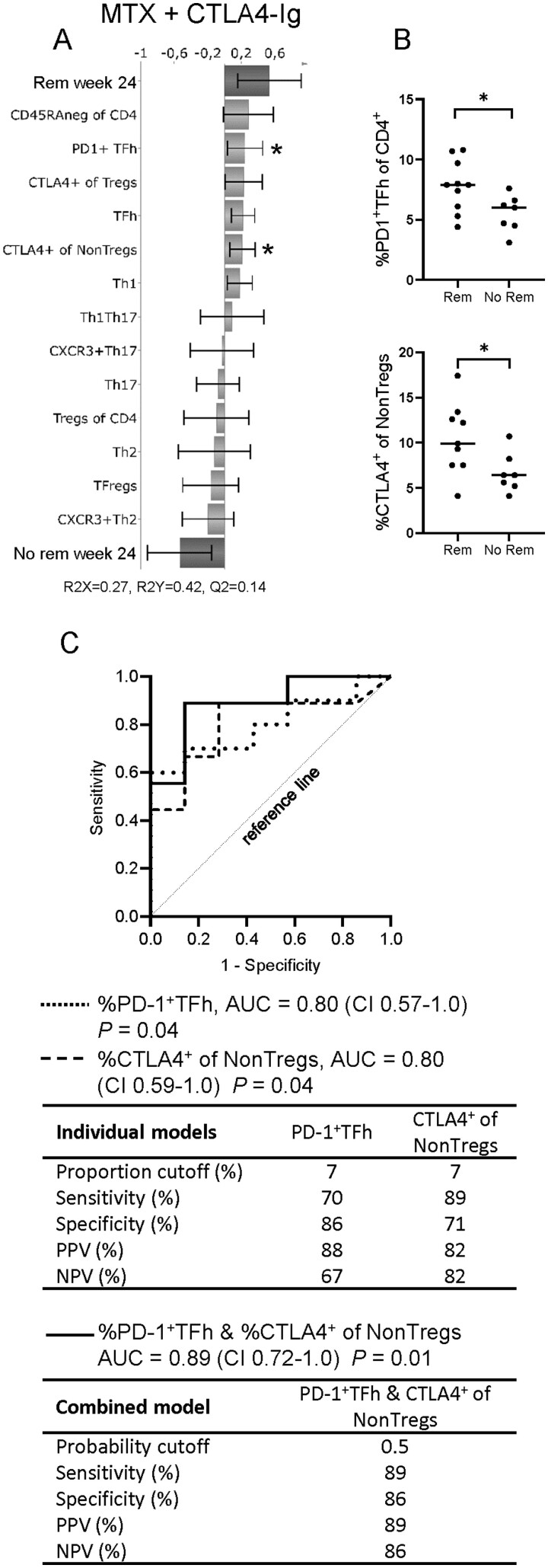
In patients treated with CTLA-4Ig, the proportions of PD-1+TFh and CTLA-4+ conventional CD4+ T cells at baseline predicted CDAI remission at week 24. CD4+ T-cell subset proportions could not predict remission after treatment with anti-IL6R or anti-TNF. The percentage of regulatory T cells (Tregs) expressing CTLA-4 decreased in all treatment arms by 24 weeks, but only CTLA-4Ig treatment significantly reduced the proportions of Tregs and PD-1+T follicular helper (TFh) cells.
These findings indicate that circulating proportions PD-1+TFh and CTLA-4+ conventional CD4+ T cells at baseline may serve as predictive biomarkers for remission in early RA after CTLA-4Ig treatment.
CTLA-4Ig 阻断 T 细胞激活,并在 RA 中具有临床疗效。然而,尚不清楚基线时血液中特定的 CD4+T 细胞亚群是否可预测 CTLA-4Ig 或其他作用机制不同的生物制剂治疗后的缓解,以及治疗如何影响未经治疗的早期 RA(eRA)患者的 CD4+T 细胞。
本研究纳入了来自更大规模随机试验的 60 例未经治疗的 eRA 患者。他们接受了甲氨蝶呤联合 CTLA-4Ig(阿巴西普,n=17)、抗 IL6 受体(托珠单抗,n=21)或抗 TNF(依那西普,n=22)治疗。通过临床疾病活动指数(CDAI)、DAS28、肿胀关节数、压痛关节数、CRP 和 ESR 评估疾病活动度。主要结局是第 24 周时 CDAI 缓解(CDAI≤2.8)。在基线和治疗 4、12 和 24 周时,通过流式细胞术测量了 12 种 CD4+T 细胞亚群的比例。
在接受 CTLA-4Ig 治疗的患者中,基线时 PD-1+TFh 和 CTLA-4+常规 CD4+T 细胞的比例可预测第 24 周时的 CDAI 缓解。抗 IL6R 或抗 TNF 治疗后,CD4+T 细胞亚群比例不能预测缓解。在所有治疗组中,24 周时调节性 T 细胞(Tregs)表达 CTLA-4 的百分比均下降,但仅 CTLA-4Ig 治疗显著降低了 Tregs 和 PD-1+T 滤泡辅助(TFh)细胞的比例。
这些发现表明,基线时循环 PD-1+TFh 和 CTLA-4+常规 CD4+T 细胞的比例可能是 CTLA-4Ig 治疗后早期 RA 缓解的预测生物标志物。