Selldén Tilia, Andersson Kerstin, Gjertsson Inger, Hultgård Ekwall Anna-Karin, Lend Kristina, Lund Hetland Merete, Østergaard Mikkel, Uhlig Tillmann, Schrumpf Heiberg Marte, Nurmohamed Michael T, Lampa Jon, Sokka Isler Tuulikki, Nordström Dan, Hørslev-Petersen Kim, Gudbjornsson Bjorn, Gröndal Gerdur, van Vollenhoven Ronald, Maglio Cristina, Lundell Anna-Carin, Rudin Anna
Department of Rheumatology and Inflammation Research, The Sahlgrenska Academy at University of Gothenburg, Gothenburg, Sweden.
Department of Rheumatology, Sahlgrenska University Hospital, Gothenburg, Sweden.
PLoS One. 2025 Aug 28;20(8):e0330823. doi: 10.1371/journal.pone.0330823. eCollection 2025.
To determine whether baseline CD4+ T helper (Th) cell subset proportions in blood may serve as predictive biomarkers for achieving remission 48 weeks after initiating CTLA-4Ig, anti-tumor necrosis factor (TNF), or anti-interleukin 6 receptor (IL6R) treatment in patients with early rheumatoid arthritis (eRA).
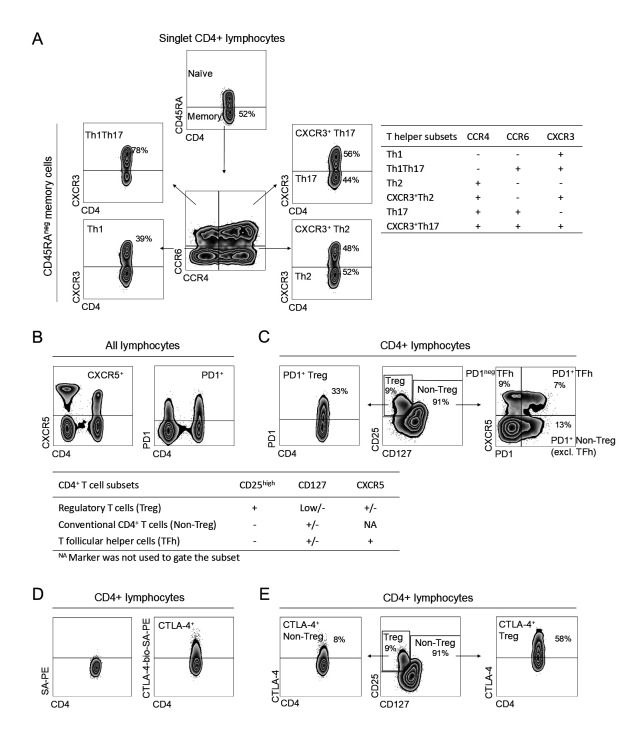
This study included 60 untreated eRA patients from the larger randomized treatment trial NORD-STAR. They were treated with methotrexate (MTX) combined with either CTLA-4Ig (n = 17), anti-TNF (n = 22), or anti-IL6R (n = 21). Disease activity was assessed by clinical disease activity index (CDAI), C-reactive protein, and erythrocyte sedimentation rate. The primary outcome was remission (CDAI ≤ 2.8) at week 48, and the secondary outcomes were time to reach remission or sustained remission during the 48-week follow-up. CD4+ T cell subset proportions were analyzed fresh by flow cytometry at baseline and at 24 and 48 weeks.
In CTLA-4Ig + MTX-treated patients, baseline Th2 together with PD1+ T follicular helper (TFh) cell proportions predicted CDAI remission at week 48 (AUC: 0.986, 95% CI 0.94-1.0). Survival analysis revealed that patients with Th2 proportions below 16.8% or PD1+ TFh proportions above 7.6% at baseline were more likely to achieve remission (log-rank p = 0.002 and p = 0.007, respectively), and sustained remission (log-rank p = 0.01 and p = 0.001, respectively), over the 48-week follow-up. CD4+ T cell subset proportions did not predict remission in patients treated with anti-TNF + MTX or anti-IL6R + MTX. Only CTLA-4Ig treatment reduced PD1+ TFh and PD1neg TFh fractions after 48 weeks.
Circulating Th2 and PD1+ TFh cell proportions at baseline may serve as predictive biomarkers for achieving CDAI remission after 48 weeks of CTLA-4Ig treatment in eRA.
确定早期类风湿性关节炎(eRA)患者在开始使用CTLA-4Ig、抗肿瘤坏死因子(TNF)或抗白细胞介素6受体(IL6R)治疗48周后实现病情缓解时,血液中的基线CD4 + T辅助(Th)细胞亚群比例是否可作为预测生物标志物。
本研究纳入了来自更大规模随机治疗试验NORD-STAR的60例未接受过治疗的eRA患者。他们接受甲氨蝶呤(MTX)联合CTLA-4Ig(n = 17)、抗TNF(n = 22)或抗IL6R(n = 21)治疗。通过临床疾病活动指数(CDAI)、C反应蛋白和红细胞沉降率评估疾病活动度。主要结局为第48周时病情缓解(CDAI≤2.8),次要结局为在48周随访期间达到缓解或持续缓解的时间。在基线、24周和48周时通过流式细胞术对CD4 + T细胞亚群比例进行新鲜样本分析。
在接受CTLA-4Ig + MTX治疗的患者中,基线Th2以及PD1 + T滤泡辅助(TFh)细胞比例可预测第48周时的CDAI缓解情况(AUC:0.986,95%CI 0.94 - 1.0)。生存分析显示,基线时Th2比例低于16.8%或PD1 + TFh比例高于7.6%的患者在48周随访期间更有可能实现缓解(对数秩检验p分别为0.002和0.007)以及持续缓解(对数秩检验p分别为0.01和0.001)。在接受抗TNF + MTX或抗IL6R + MTX治疗的患者中,CD4 + T细胞亚群比例不能预测缓解情况。仅CTLA-4Ig治疗在48周后降低了PD1 + TFh和PD1neg TFh比例。
基线时循环Th2和PD1 + TFh细胞比例可作为eRA患者接受CTLA-4Ig治疗48周后实现CDAI缓解的预测生物标志物。