D'Amore Francesco, Grinberg Farida, Mauler Jörg, Galldiks Norbert, Blazhenets Ganna, Farrher Ezequiel, Filss Christian, Stoffels Gabriele, Mottaghy Felix M, Lohmann Philipp, Shah Nadim Jon, Langen Karl-Josef
Institute of Neuroscience and Medicine, Research Centre Juelich, Juelich, Germany.
Department of Neuroradiology, Circolo Hospital and Macchi Foundation, Varese, Italy.
Neurooncol Adv. 2021 Mar 10;3(1):vdab044. doi: 10.1093/noajnl/vdab044. eCollection 2021 Jan-Dec.
Radiological differentiation of tumor progression (TPR) from treatment-related changes (TRC) in pretreated glioblastoma is crucial. This study aimed to explore the diagnostic value of diffusion kurtosis MRI combined with information derived from -(2-[F]-fluoroethyl)-l-tyrosine (F-FET) PET for the differentiation of TPR from TRC in patients with pretreated glioblastoma.
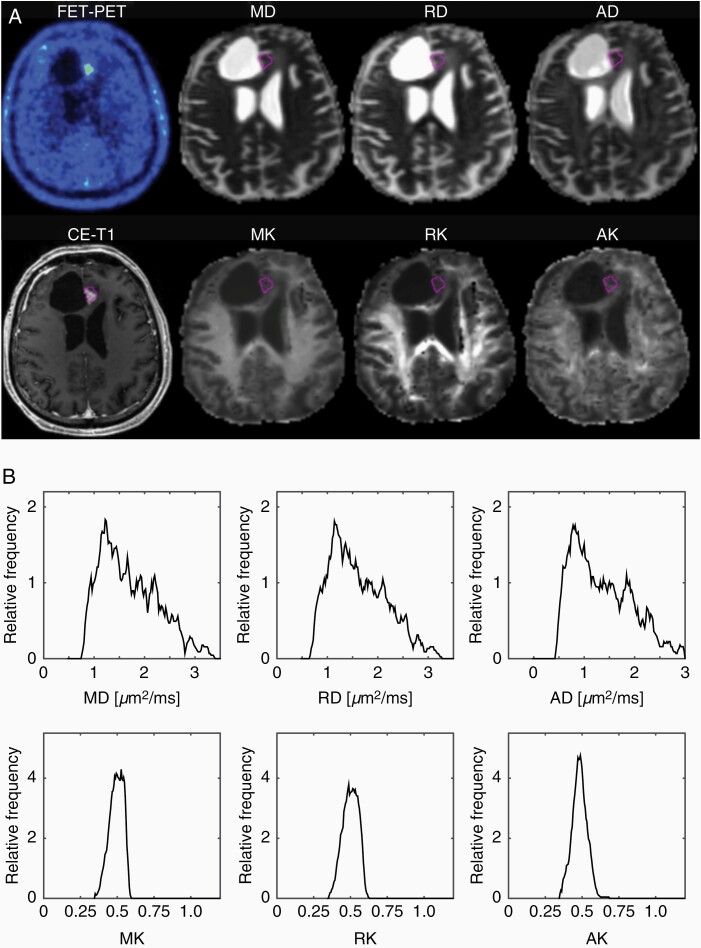
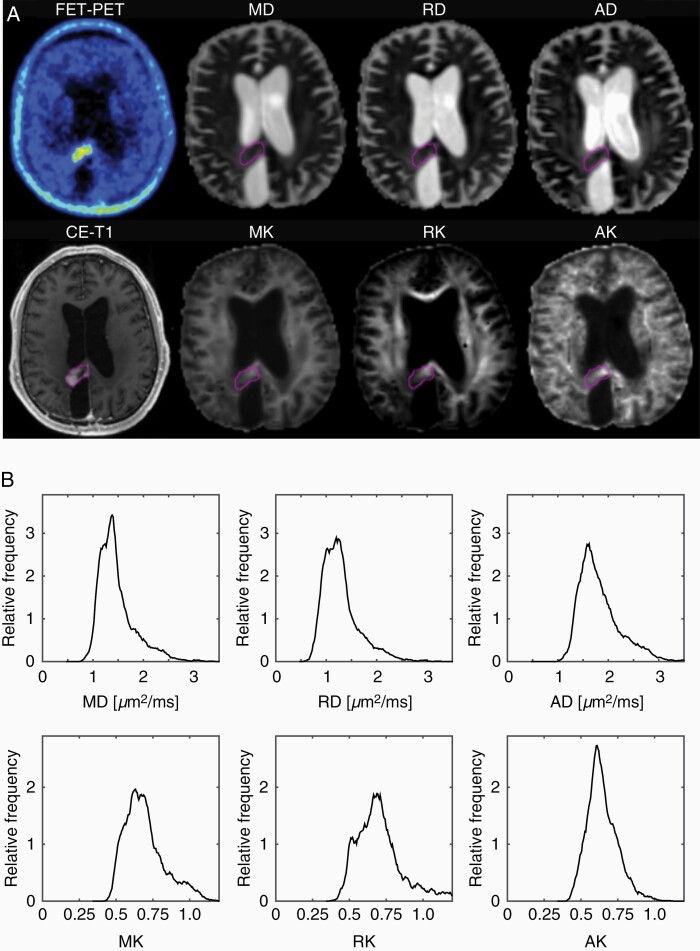
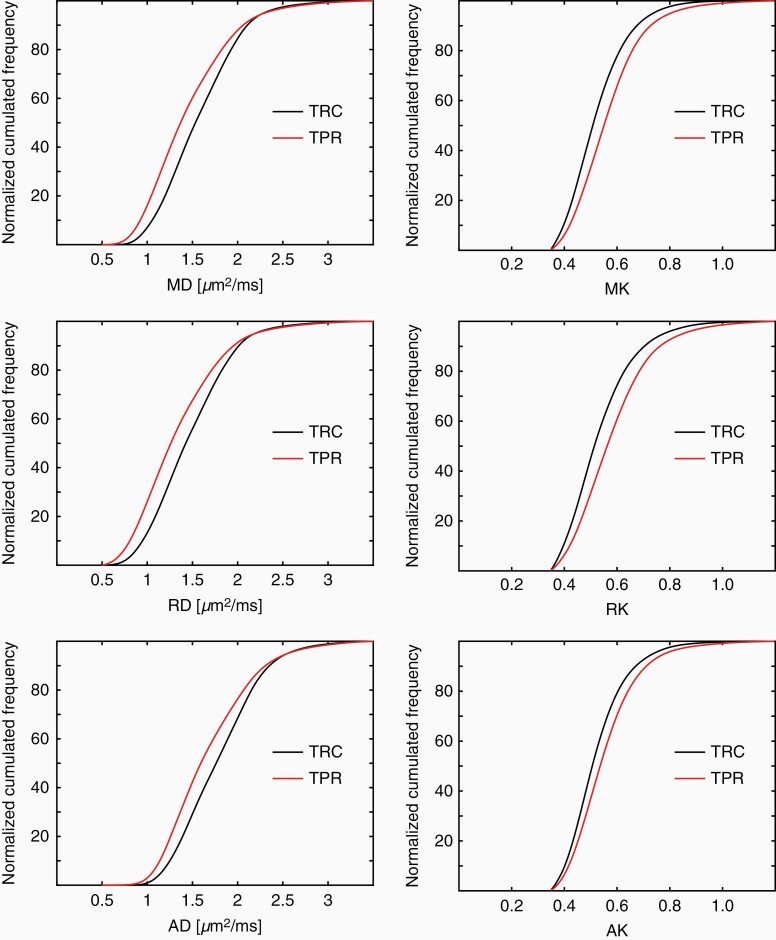
Thirty-two patients with histomolecularly defined and pretreated glioblastoma suspected of having TPR were included in this retrospective study. Twenty-one patients were included in the TPR group, and 11 patients in the TRC group, as assessed by neuropathology or clinicoradiological follow-up. Three-dimensional (3D) regions of interest were generated based on increased F-FET uptake using a tumor-to-brain ratio of 1.6. Furthermore, diffusion MRI kurtosis maps were obtained from the same regions of interest using co-registered F-FET PET images, and advanced histogram analysis of diffusion kurtosis map parameters was applied to generated 3D regions of interest. Diagnostic accuracy was analyzed by receiver operating characteristic curve analysis and combinations of PET and MRI parameters using multivariate logistic regression.
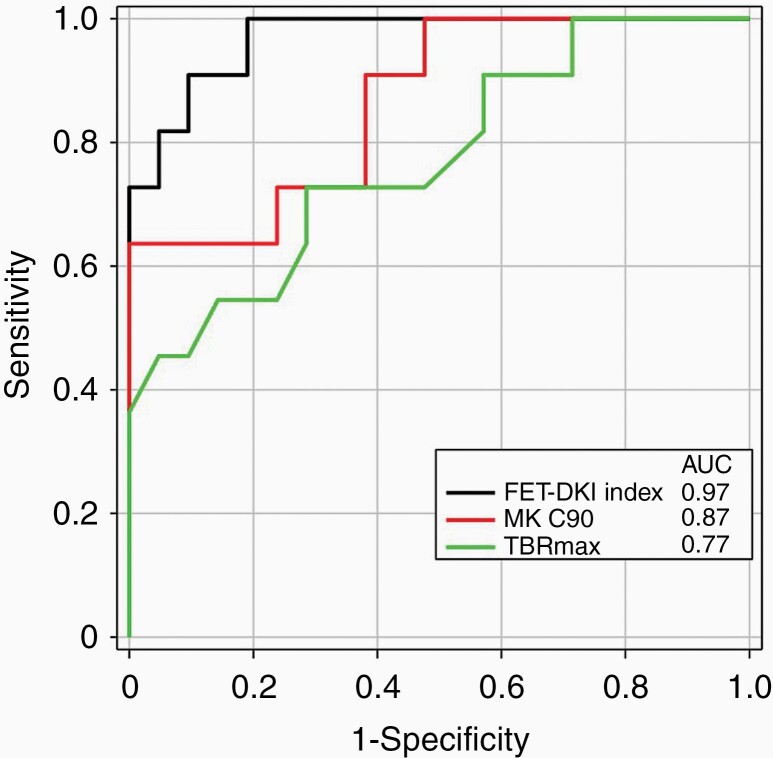
Parameters derived from diffusion MRI kurtosis maps show high diagnostic accuracy, up to 88%, for differentiating between TPR and TRC. Logistic regression revealed that the highest diagnostic accuracy of 94% (area under the curve, 0.97; sensitivity, 94%; specificity, 91%) was achieved by combining the maximum tumor-to-brain ratio of F-FET uptake and diffusion MRI kurtosis metrics.
The combined use of F-FET PET and MRI diffusion kurtosis maps appears to be a promising approach to improve the differentiation of TPR from TRC in pretreated glioblastoma and warrants further investigation.
在预处理的胶质母细胞瘤中,从治疗相关变化(TRC)中进行肿瘤进展(TPR)的放射学鉴别至关重要。本研究旨在探讨扩散峰度MRI联合源自[18F] -氟代乙基-L-酪氨酸(F-FET)PET的信息在预处理胶质母细胞瘤患者中区分TPR与TRC的诊断价值。
本回顾性研究纳入了32例组织分子学明确且疑似存在TPR的预处理胶质母细胞瘤患者。经神经病理学或临床放射学随访评估,TPR组纳入21例患者,TRC组纳入11例患者。基于F-FET摄取增加,使用肿瘤与脑的比值为1.6生成三维(3D)感兴趣区。此外,使用配准的F-FET PET图像从相同的感兴趣区获取扩散MRI峰度图,并对扩散峰度图参数进行高级直方图分析以生成3D感兴趣区。通过受试者工作特征曲线分析以及使用多变量逻辑回归的PET和MRI参数组合来分析诊断准确性。
扩散MRI峰度图得出的参数在区分TPR和TRC方面显示出高达88%的高诊断准确性。逻辑回归显示将F-FET摄取的最大肿瘤与脑比值和扩散MRI峰度指标相结合可实现最高94%的诊断准确性(曲线下面积为0.97;敏感性为94%;特异性为91%)。
联合使用F-FET PET和MRI扩散峰度图似乎是一种有前景的方法,可改善预处理胶质母细胞瘤中TPR与TRC的鉴别,值得进一步研究。