Fukui Yasuhiro, Kubo Naoshi, Sakurai Katsunobu, Tamamori Yutaka, Maeda Kiyoshi, Ohira Masaichi
Department of Gastroenterological Surgery, Osaka City General Hospital, 2-13-22 Miyakojima-hondori Miyakojima-ku, Osaka City, Osaka, 534-0021, Japan.
Department of Surgery, Osaka City University Graduate School of Medicine, 1-4-3 Asahi-machi, Abeno-ku, Osaka-City, Osaka, 545-8585, Japan.
Surg Case Rep. 2021 May 19;7(1):124. doi: 10.1186/s40792-021-01202-x.
Port site metastasis (PSM) after curative gastrectomy for gastric cancer and muscular metastasis from gastric cancer are rare manifestations. Similarly, subcutaneous metastasis from gastric cancer is rare, and muscular and subcutaneous metastases are associated with poor prognosis. We report a case of long-term survival in a patient who underwent curative resection of gastric cancer and repeated recurrence of port site, muscular and subcutaneous metastases from gastric cancer, treated by resection.
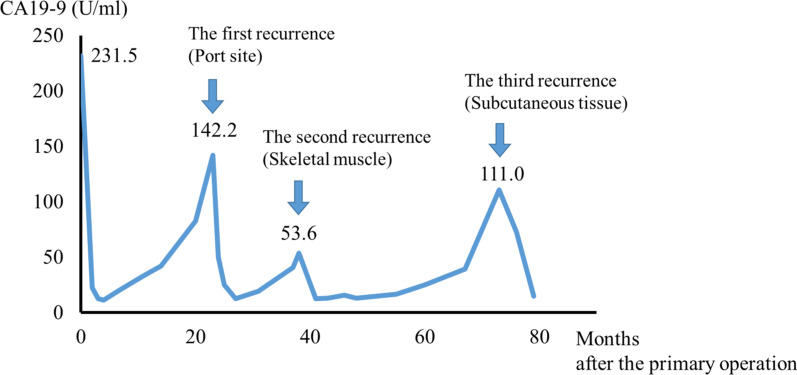
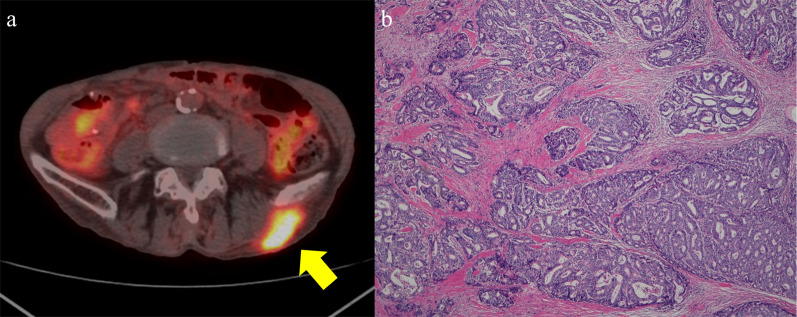
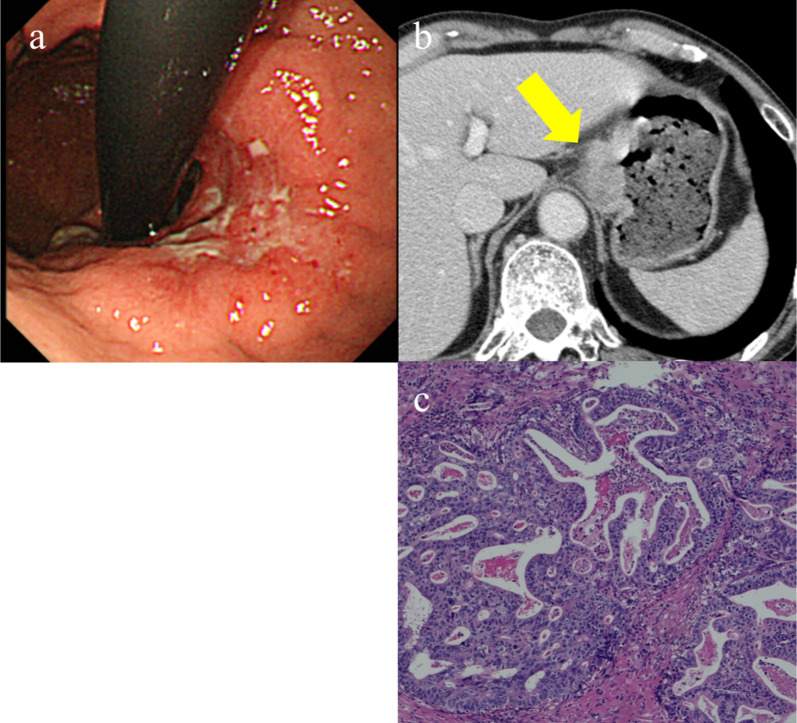
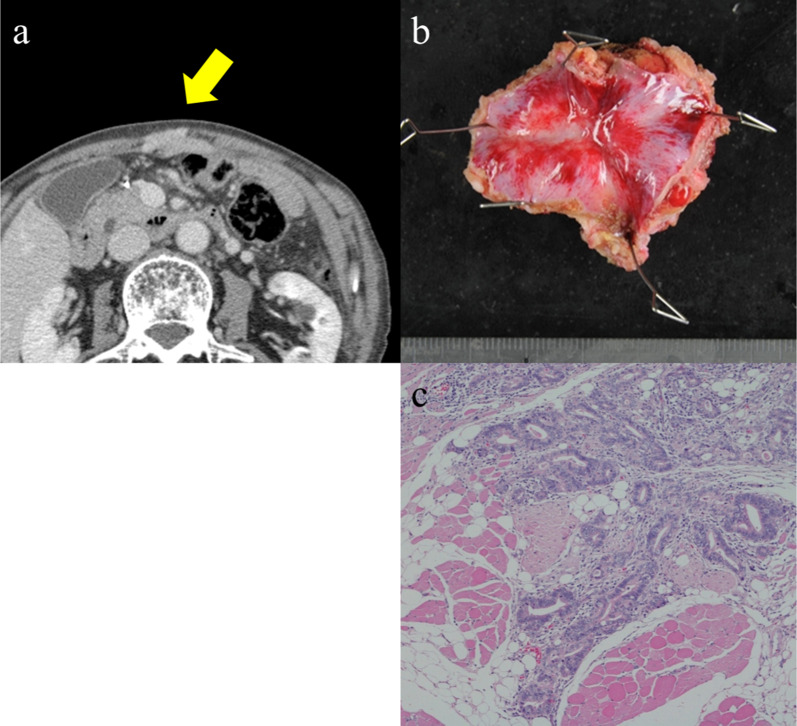
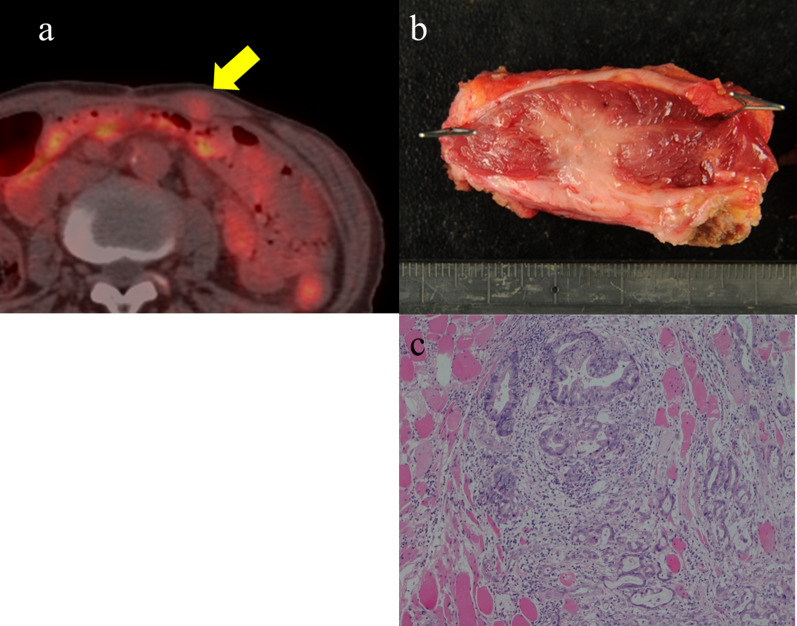
A 75-year-old man was diagnosed with gastric cancer and referred to our department. Upper endoscopy demonstrated a 5-cm circumferential ulcerated lesion at the cardia. Biopsy findings showed a poorly differentiated tubular adenocarcinoma. He underwent laparoscopic total gastrectomy with lymph node dissection, and pathologic examination revealed a moderately differentiated tubular adenocarcinoma stage T4aN1M0 and IIIA according to the UICC (Union for International Cancer Control) classification. He refused adjuvant chemotherapy and was only carefully observed. Twenty-three months after the primary gastrectomy, computed tomography (CT) revealed an irregular mass near the port site wounds. Then the patient underwent mass resection, and the pathological diagnosis was consistent with metastatic adenocarcinoma, located in the subcutaneous tissue at the port site wounds. Thirteen months after the second surgery, CT revealed an enhanced mass in the abdominal wall. Positron emission tomography (PET) CT showed an elevated uptake in the rectus abdominis muscle and a standardized uptake value (SUV) of 3.1. The patient underwent another mass resection, and the pathological diagnosis was consistent with metastatic adenocarcinoma in the rectus abdominis muscle. Thirty-five months after the third surgery, CT revealed a mass in the left gluteal subcutaneous region. Furthermore, PET-CT revealed a 35-mm mass with an elevated SUV of 9.6. Another mass resection procedure was performed, and the pathological diagnosis was consistent with metastatic adenocarcinoma in the subcutaneous tissue. Since tumor cells were present at the resection margin, additional radiation therapy was performed. The patient has survived 78 months after primary gastrectomy.
The prognosis of muscular and subcutaneous metastases from gastric cancer is poor. However, if the metastatic tumor is solitary, surgical excision could be a feasible treatment option and might prolong survival.
胃癌根治性胃切除术后的切口种植转移(PSM)以及胃癌的肌肉转移是罕见的表现。同样,胃癌的皮下转移也很罕见,肌肉和皮下转移与预后不良相关。我们报告一例接受胃癌根治性切除术后出现切口种植、肌肉和皮下转移反复复发并经手术切除治疗后长期存活的患者。
一名75岁男性被诊断为胃癌并转诊至我科。上消化道内镜检查显示贲门处有一个5厘米的环形溃疡病变。活检结果显示为低分化管状腺癌。他接受了腹腔镜全胃切除术及淋巴结清扫术,病理检查根据国际癌症控制联盟(UICC)分类显示为中分化管状腺癌,T4aN1M0期,IIIA期。他拒绝辅助化疗,仅接受密切观察。初次胃切除术后23个月,计算机断层扫描(CT)显示切口附近有一个不规则肿块。随后患者接受了肿块切除术,病理诊断为转移性腺癌,位于切口处皮下组织。第二次手术后13个月,CT显示腹壁有一个强化肿块。正电子发射断层扫描(PET)CT显示腹直肌摄取增加,标准化摄取值(SUV)为3.1。患者接受了另一次肿块切除术,病理诊断为腹直肌转移性腺癌。第三次手术后35个月,CT显示左臀皮下区域有一个肿块。此外,PET-CT显示一个35毫米的肿块,SUV升高至9.6。又进行了一次肿块切除手术,病理诊断为皮下组织转移性腺癌。由于切除边缘存在肿瘤细胞,因此进行了额外的放射治疗。患者在初次胃切除术后已存活78个月。
胃癌肌肉和皮下转移的预后较差。然而,如果转移瘤为孤立性,手术切除可能是一种可行的治疗选择,并且可能延长生存期。