Department of Medicine Mayo Clinic Rochester MN.
Department of Cardiovascular Surgery Mayo Clinic Rochester MN.
J Am Heart Assoc. 2021 Jun;10(11):e019907. doi: 10.1161/JAHA.120.019907. Epub 2021 May 20.
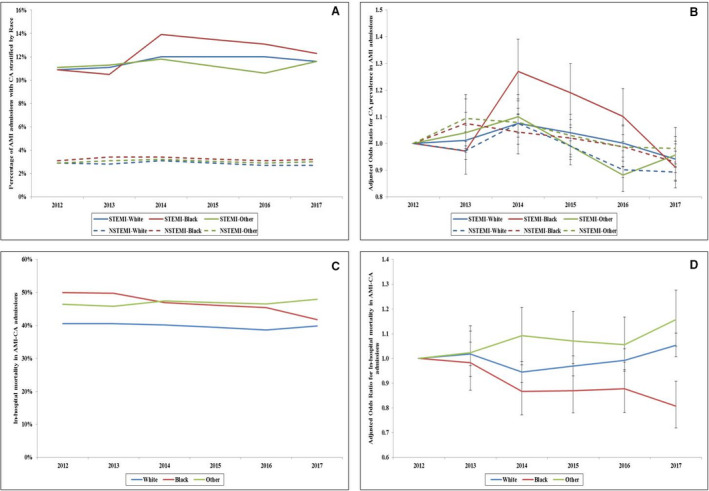
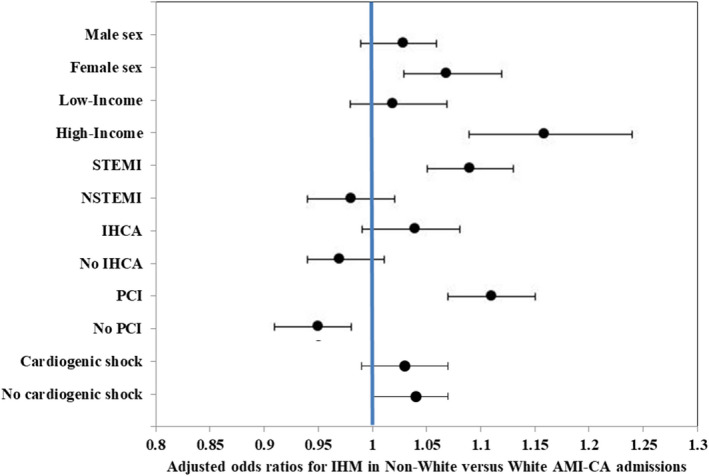
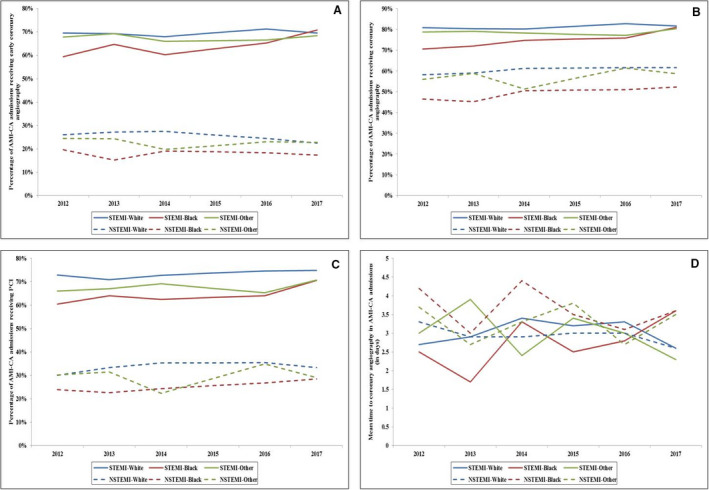
Background The role of race and ethnicity in the outcomes of cardiac arrest (CA) complicating acute myocardial infarction (AMI) is incompletely understood. Methods and Results This was a retrospective cohort study of adult admissions with AMI-CA from the National Inpatient Sample (2012-2017). Self-reported race/ethnicity was classified as White, Black, and others (Hispanic, Asian or Pacific Islander, Native American, Other). Outcomes of interest included in-hospital mortality, coronary angiography, percutaneous coronary intervention, palliative care consultation, do-not-resuscitate status use, hospitalization costs, hospital length of stay, and discharge disposition. Of the 3.5 million admissions with AMI, CA was noted in 182 750 (5.2%), with White, Black, and other races/ethnicities constituting 74.8%, 10.7%, and 14.5%, respectively. Black patients admitted with AMI-CA were more likely to be female, with more comorbidities, higher rates of non-ST-segment-elevation myocardial infarction, and higher neurological and renal failure. Admissions of patients of Black and other races/ethnicities underwent coronary angiography (61.9% versus 70.2% versus 73.1%) and percutaneous coronary intervention (44.6% versus 53.0% versus 58.1%) less frequently compared to patients of white race (<0.001). Admissions of patients with AMI-CA had significantly higher unadjusted mortality (47.4% and 47.4%) as compared with White patients admitted (40.9%). In adjusted analyses, Black race was associated with lower in-hospital mortality (odds ratio [OR], 0.95; 95% CI, 0.91-0.99; =0.007) whereas other races had higher in-hospital mortality (OR, 1.11; 95% CI, 1.08-1.15; <0.001) compared with White race. Admissions of Black patients with AMI-CA had longer length of hospital stay, higher rates of palliative care consultation, less frequent do-not-resuscitate status use, and fewer discharges to home (all <0.001). Conclusions Racial and ethnic minorities received less frequent guideline-directed procedures and had higher in-hospital mortality and worse outcomes in AMI-CA.
背景 种族和民族在急性心肌梗死(AMI)并发心搏骤停(CA)的结果中的作用尚不完全清楚。
方法和结果 这是一项对 2012 年至 2017 年期间国家住院患者样本(National Inpatient Sample)中成人 AMI-CA 住院患者的回顾性队列研究。自我报告的种族/民族分为白人、黑人以及其他(西班牙裔、亚洲或太平洋岛民、美国原住民、其他)。感兴趣的结果包括院内死亡率、冠状动脉造影、经皮冠状动脉介入治疗、姑息治疗咨询、不复苏状态使用、住院费用、住院时间和出院去向。在 350 万例 AMI 住院患者中,有 182750 例(5.2%)发生 CA,白人、黑人、其他种族/民族分别占 74.8%、10.7%和 14.5%。患有 AMI-CA 的黑人患者更可能是女性,合并症更多,非 ST 段抬高型心肌梗死发生率更高,以及神经和肾功能衰竭发生率更高。与白人患者相比(<0.001),黑人患者和其他种族/民族患者接受冠状动脉造影(61.9%、61.9%和 73.1%)和经皮冠状动脉介入治疗(44.6%、44.6%和 58.1%)的比例较低。与白人患者相比,患有 AMI-CA 的患者的死亡率明显更高(47.4%和 47.4%)。在调整后的分析中,与白人患者相比,黑人种族与较低的院内死亡率相关(比值比[OR],0.95;95%置信区间,0.91-0.99;=0.007),而其他种族的院内死亡率更高(OR,1.11;95%置信区间,1.08-1.15;<0.001)。患有 AMI-CA 的黑人患者住院时间更长,姑息治疗咨询率更高,不复苏状态使用频率更低,出院回家的患者更少(均<0.001)。
结论 少数民族接受的指南推荐治疗程序较少,院内死亡率较高,AMI-CA 结局较差。