Skeletal Dysplasia Program, Division of Orthogenetics, Nemours/Alfred I. duPont Hospital for Children, 1600 Rockland Road, Wilmington, DE, 19803, USA.
Department of Research, Nemours/Alfred I. duPont Hospital for Children, Wilmington, DE, USA.
Orphanet J Rare Dis. 2021 May 20;16(1):231. doi: 10.1186/s13023-021-01852-y.
Microcephalic osteodysplastic primordial dwarfism type II (MOPDII) is the most common form of primordial dwarfism, caused by bialleic mutations in the pericentrin gene (PCNT). Aside from its classic features, there are multiple associated medical complications, including a well-documented risk of neurovascular disease. Over the past several years, it has become apparent that additional vascular issues, as well as systemic hypertension and kidney disease may also be related to MOPDII. However, the frequency and extent of the vasculopathy was unclear. To help address this question, a vascular substudy was initiated within our Primordial Dwarfism Registry.
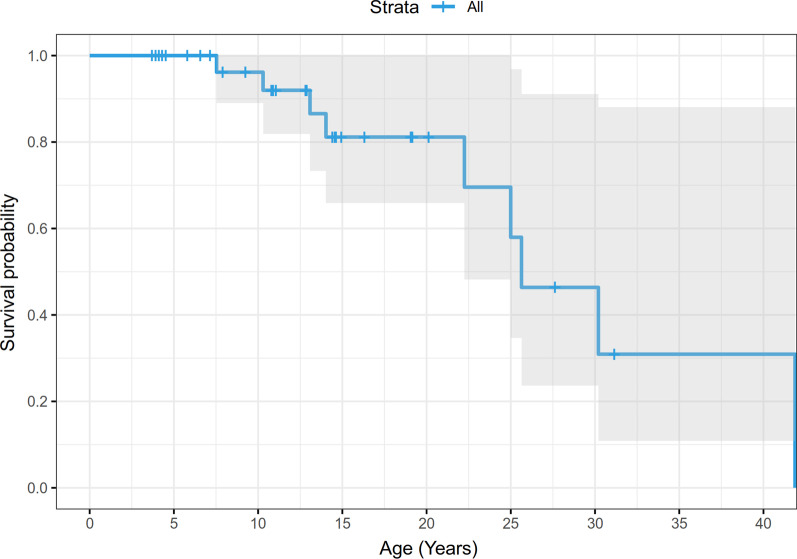
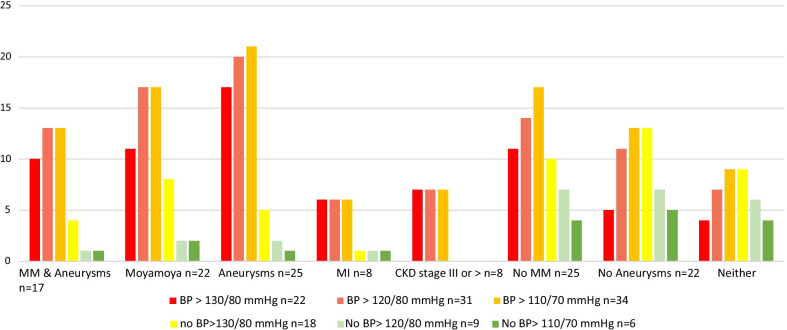
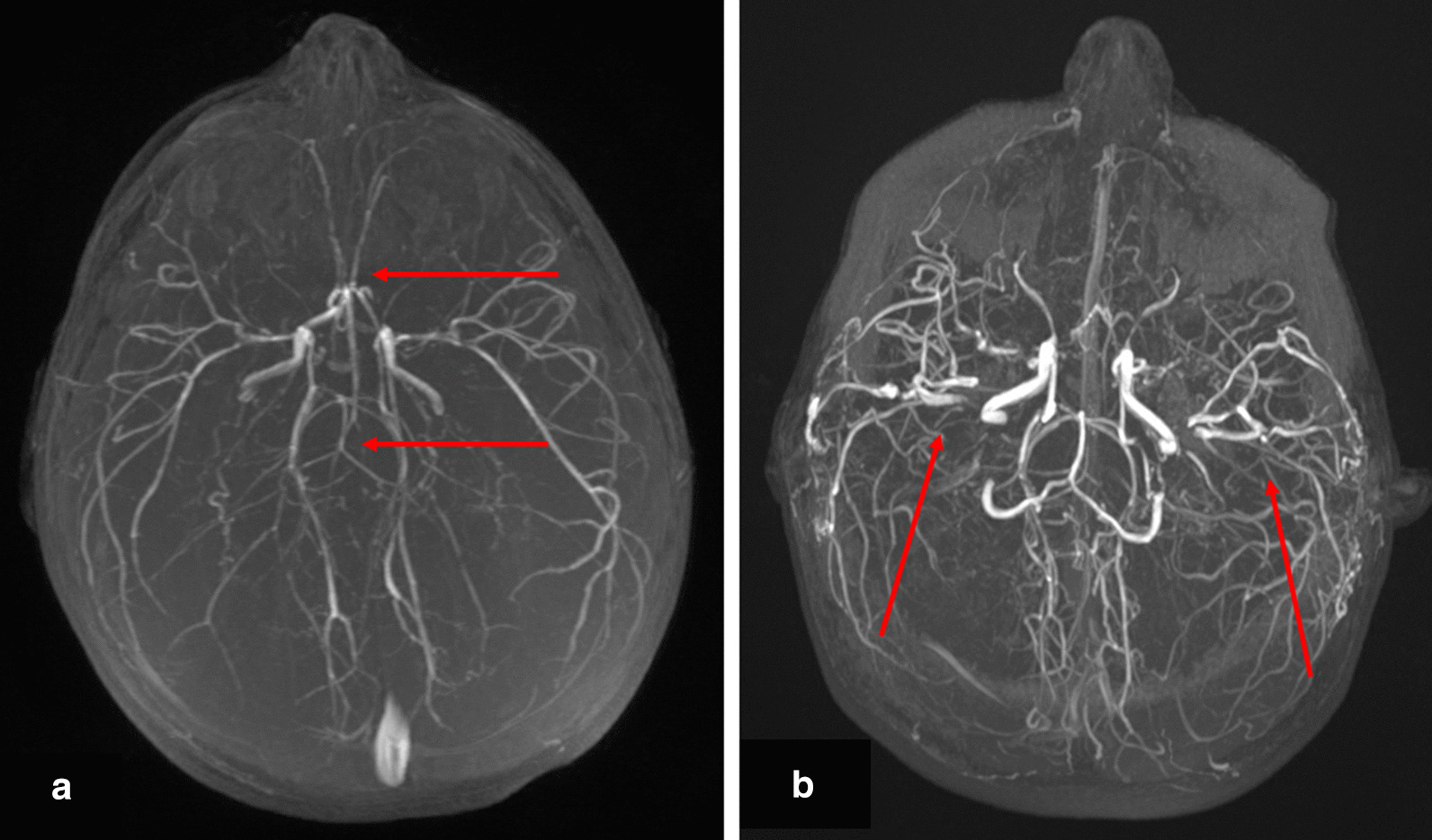
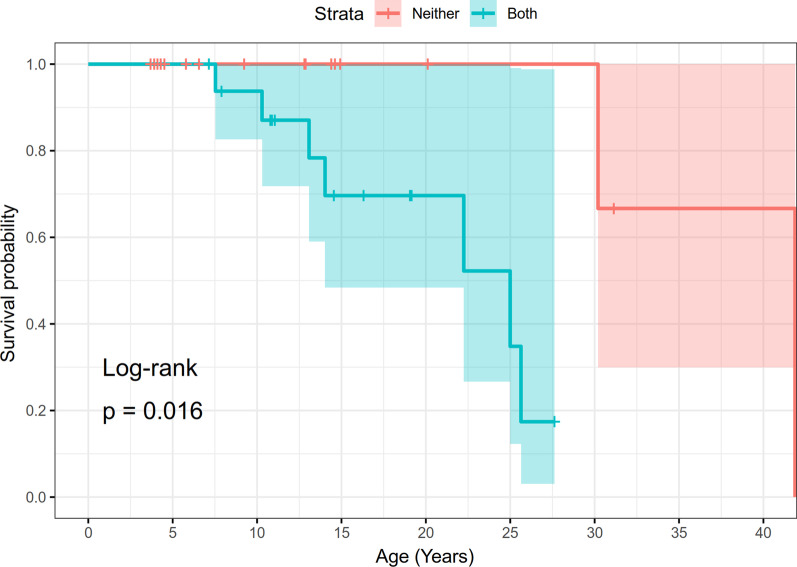
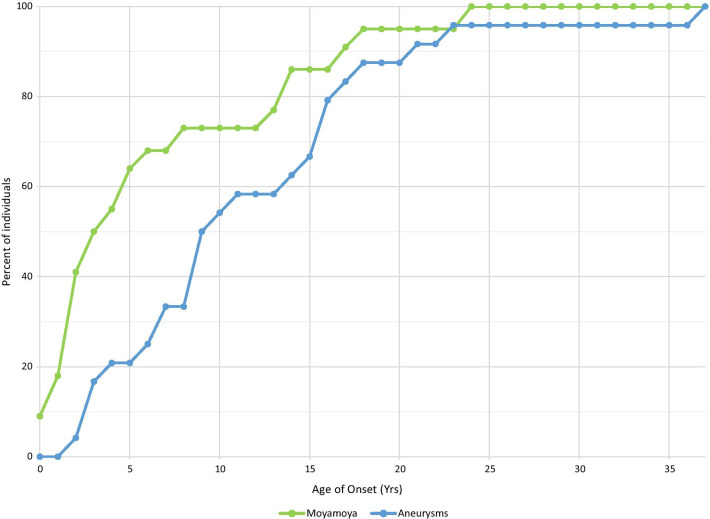
Medical records from 47 individuals, living and deceased, ranging in age from 3 to 41 years of age were interrogated for this purpose. Of the total group, 64% were diagnosed with moyamoya, intracranial aneurysms, or both. In general, the age at diagnosis for moyamoya was younger than aneurysms, but the risk for neurovascular disease was throughout the shortened lifespan. In addition to neurovascular disease, renal, coronary and external carotid artery involvement are documented. 43% of the total group was diagnosed with hypertension, and 17% had myocardial infarctions. A total of 32% of the entire cohort had some form of chronic kidney disease, with 4% of the total group necessitating a kidney transplant. In addition, 38% had diabetes/insulin resistance. Ages of diagnoses, treatment modalities employed, and location of vasculopathies were notated as available and applicable, as well as frequencies of other comorbidities.
It is now clear that vascular disease in MOPDII is global and screening of the cardiac and renal vessels is warranted along with close monitoring of blood pressure. We recommend a blood pressure of 110/70 mmHg as a starting point for an upper limit, especially if the individual has a history of neurovascular disease, chronic kidney disease and/or diabetes. Additionally, providers need to be at high alert for the possibility of myocardial infarctions in young adults with MOPDII, so that appropriate treatment can be initiated promptly in an acute situation.
小头-骨-发育不良性矮小症 II 型(MOPDII)是最常见的矮小症,由中心体蛋白基因(PCNT)的双等位基因突变引起。除了其典型特征外,还有多种相关的医疗并发症,包括已被充分记录的神经血管疾病风险。在过去的几年中,人们已经清楚地认识到,MOPDII 还可能与其他血管问题以及系统性高血压和肾脏疾病有关。然而,血管病变的频率和程度尚不清楚。为了帮助解决这个问题,我们在原发性矮小症登记处启动了一项血管子研究。
为此目的,对 47 名年龄在 3 至 41 岁之间的活人和已故个体的医疗记录进行了调查。在总人群中,64%被诊断为烟雾病、颅内动脉瘤或两者兼有。一般来说,烟雾病的诊断年龄比动脉瘤小,但神经血管疾病的风险贯穿于缩短的寿命。除了神经血管疾病外,还记录了肾脏、冠状动脉和颈外动脉的受累情况。总人群中有 43%被诊断为高血压,17%患有心肌梗死。共有 32%的总队列患有某种形式的慢性肾脏疾病,其中 4%的总队列需要进行肾脏移植。此外,38%患有糖尿病/胰岛素抵抗。记录了所有血管病变的诊断年龄、采用的治疗方式以及血管病变的位置,并记录了其他合并症的频率。
现在很清楚,MOPDII 中的血管疾病是全身性的,需要对心脏和肾脏血管进行筛查,并密切监测血压。我们建议将 110/70mmHg 作为上限的起始血压,特别是如果个体有神经血管疾病、慢性肾脏疾病和/或糖尿病病史。此外,提供者需要高度警惕 MOPDII 年轻成年人发生心肌梗死的可能性,以便在急性情况下及时启动适当的治疗。