Department of Urology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Department of Pathology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Technol Cancer Res Treat. 2021 Jan-Dec;20:15330338211019507. doi: 10.1177/15330338211019507.
The relationship between the size of the primary tumor and the prognosis of patients with metastatic renal cell carcinoma (mRCC) is unclear. In this study, we aimed to investigate the significance of the size of the primary tumor in mRCC.
We retrospectively reviewed the data of patients with mRCC who underwent cytoreductive nephrectomy (CN) from 2006 to 2013 in a Chinese center (n = 96) and those in the Surveillance, Epidemiology, and End Results (SEER) database (from 2004 to 2015, n = 4403). Tumors less than 4 cm in size were defined as small. Prognostic factors were analyzed using univariate and multivariate Cox proportional hazards regression analyses.
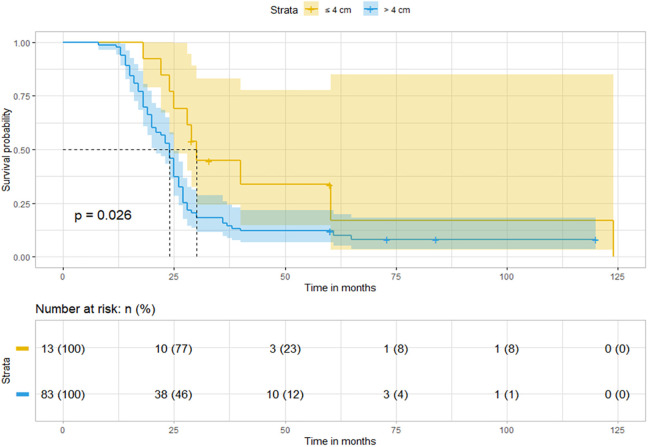
Patients with small tumors had a longer overall survival than other patients, both in the Chinese cohort (median, 30.0 vs 24.0 months, = 0.026) and the SEER cohort (median, 43.0 vs 23.0 months, < 0.001). After adjusting for other significant prognostic factors, small tumor size was still an independent protective factor in the Chinese cohort (adjusted hazard ratio [HR], 0.793; 95% confidence interval [CI]: 0.587-0.998, = 0.043). In the SEER cohort, multivariate analysis showed that small tumor size was also an independent protective factor (HR, 0.880; 95% CI: 0.654-0.987, = 0.008). In addition, as a continuous variable, a 1 cm elevation in tumor size translated into a 3.8% higher risk of death (HR, 1.038; 95% CI, 1.029-1.046; < 0.001).
Patients with small tumors may have a favorable prognosis after CN for mRCC. Although CN is not a standard protocol in mRCC, small tumor size may be a candidate when we are deciding to perform CN because of the potential benefit for OS.
原发肿瘤大小与转移性肾细胞癌(mRCC)患者的预后之间的关系尚不清楚。本研究旨在探讨 mRCC 中原发肿瘤大小的意义。
我们回顾性分析了 2006 年至 2013 年间在中国中心接受细胞减灭性肾切除术(CN)的 mRCC 患者(n = 96)和 SEER 数据库(2004 年至 2015 年,n = 4403)的数据。肿瘤小于 4cm 定义为小肿瘤。采用单因素和多因素 Cox 比例风险回归分析来分析预后因素。
在中国队列中(中位数,30.0 与 24.0 个月, = 0.026)和 SEER 队列中(中位数,43.0 与 23.0 个月, < 0.001),小肿瘤患者的总生存期均长于其他患者。在调整其他重要预后因素后,小肿瘤大小在中国人队列中仍然是独立的保护因素(调整后的风险比[HR],0.793;95%置信区间[CI]:0.587-0.998, = 0.043)。在 SEER 队列中,多因素分析表明,小肿瘤大小也是独立的保护因素(HR,0.880;95%CI:0.654-0.987, = 0.008)。此外,作为一个连续变量,肿瘤大小增加 1cm,死亡风险增加 3.8%(HR,1.038;95%CI,1.029-1.046; < 0.001)。
CN 治疗 mRCC 后,小肿瘤患者可能有较好的预后。尽管 CN 不是 mRCC 的标准方案,但由于 OS 获益的潜力,小肿瘤大小可能是进行 CN 的候选因素。