Du Er-Zhu, Liu Wei-Hong, Wáng Yì Xiáng J
Department of Radiology, Dongguan Traditional Chinese Medicine Hospital, Dongguan, Guangdong province, China.
Department of Radiology, General Hospital of China Resources & Wuhan Iron and Steel Corporation, Wuhan, Hubei province, China.
J Orthop Translat. 2021 May 5;28:169-178. doi: 10.1016/j.jot.2021.04.001. eCollection 2021 May.
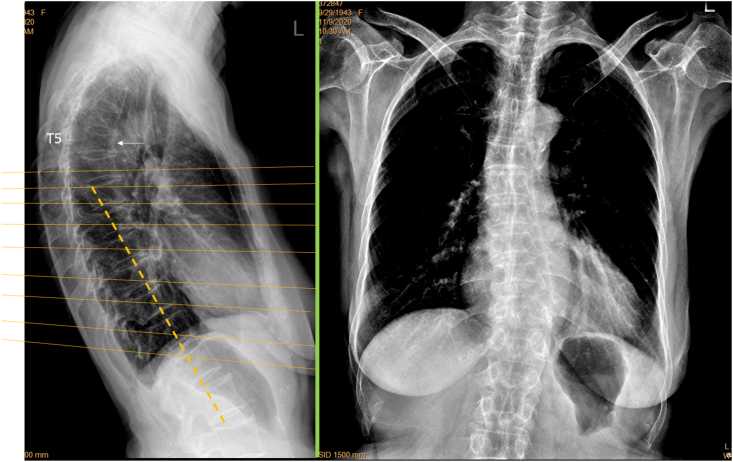
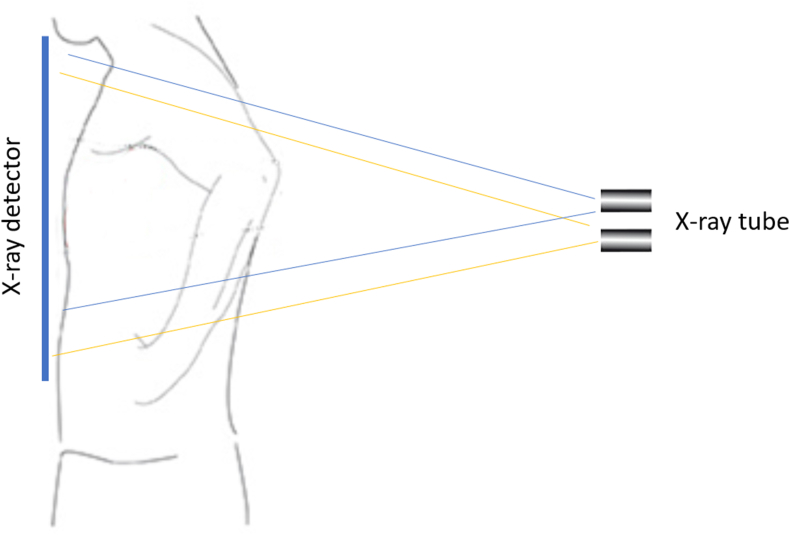
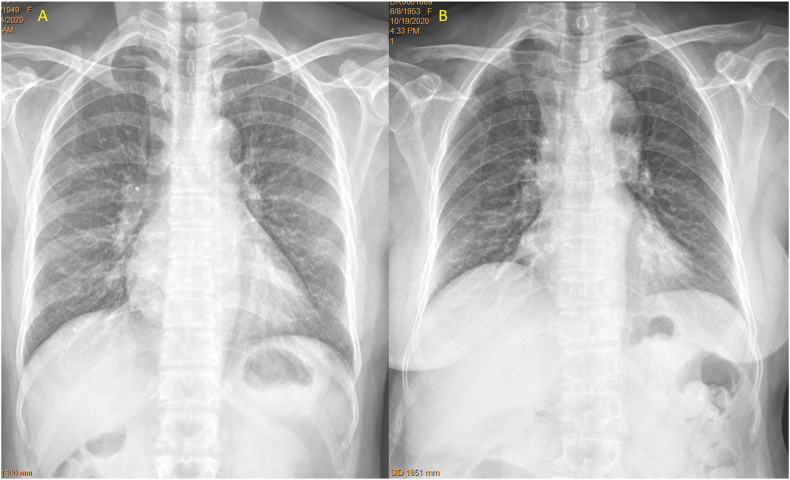
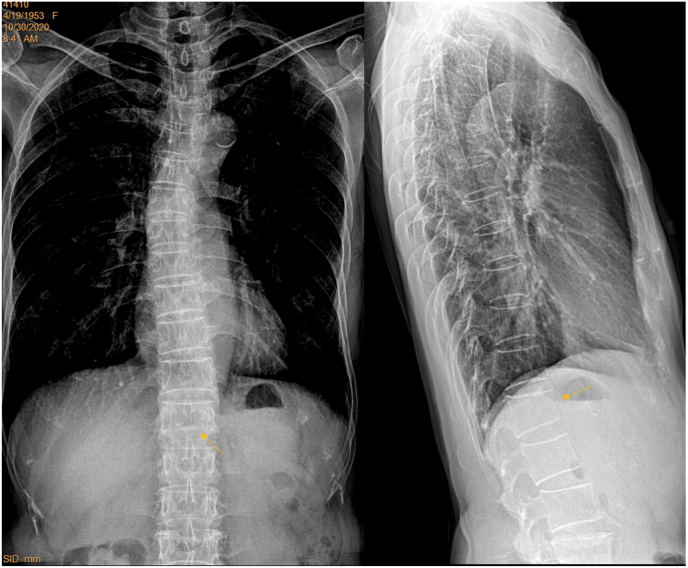
In clinics, chest frontal view radiograph (CFR) is often taken for patients suspected of respiratory diseases and for assessing the heart and big vessels. CFR can be utilised to opportunistically detect osteoporotic vertebral fracture (OVF). However, for standard CFR, the site of highest OVF prevalence, i.e., the thoracolumbar junction, is usually 'off-centre' to the X-ray beam focus. This study tested the hypothesis that, if a CRF is taken with approximately two vertebrae lower than the standard X-ray beam positioning, the visualization of thoraco-lumbar junction can be much improved.
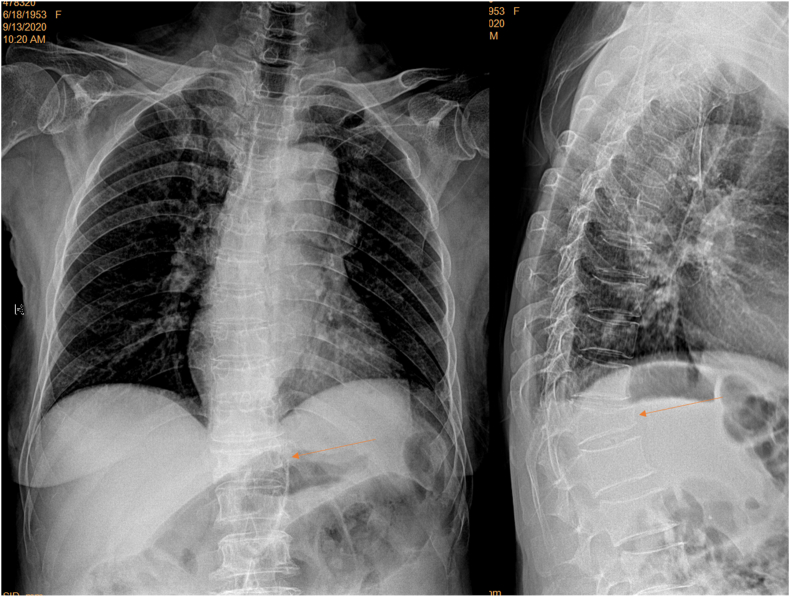
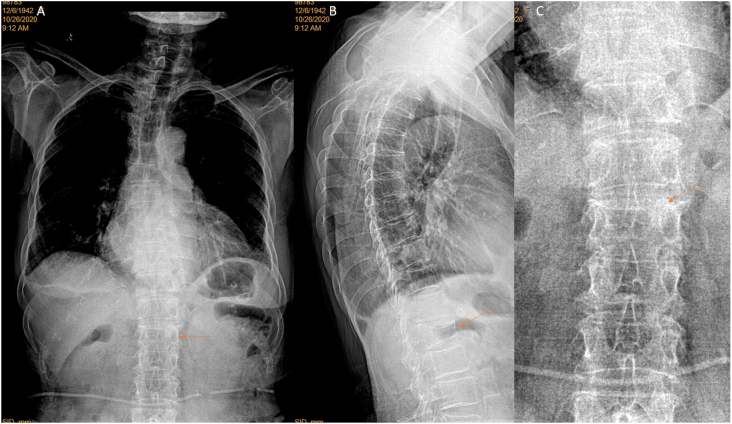
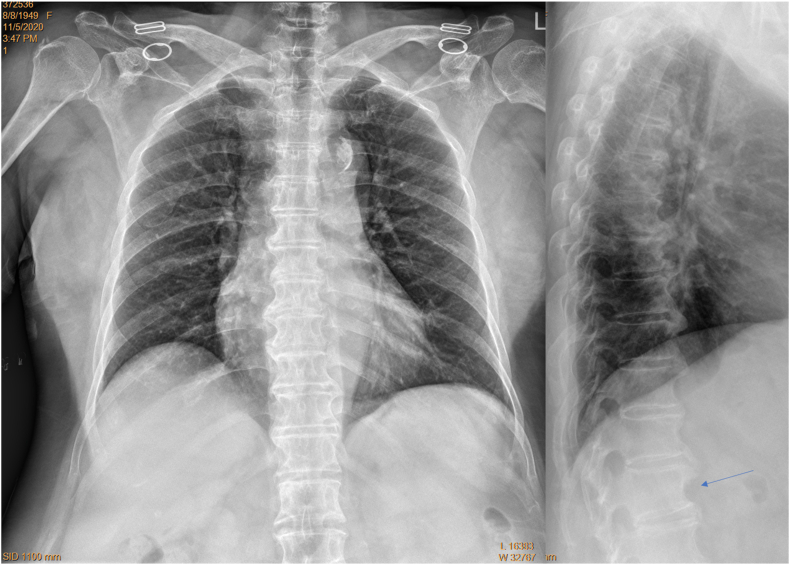
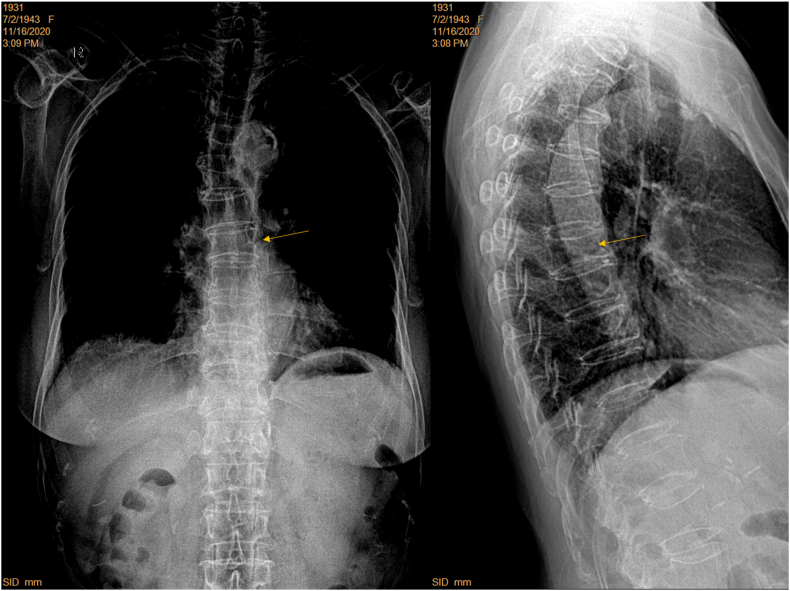
Four hospitals (A, B, C, D) provided 101 elderly women's digital CFRs with standard filming (28, 20, 24, and 21 cases respectively). Eighty four elderly female patients were prospectively recruited from hospitals-A and B, who were consecutive patients referred for chest radiograph with indications other than spine disorders. For theses prospective CFRs, the focus of X-ray beam was adjusted from towards vertebra T6 to towards T8, and standard lateral radiographs were obtained for reference. Visibility of spine and detectability of OVF were assessed on the CFRs. OVF was diagnosed based on chest lateral radiograph (CLR) after excluding other potential causes both radiographically and clinically.
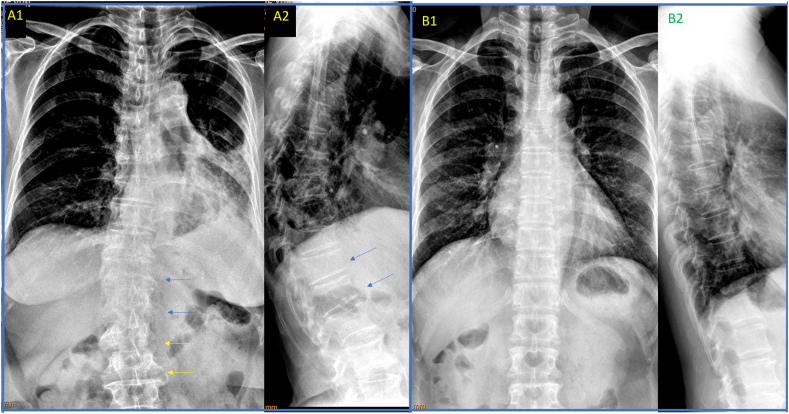
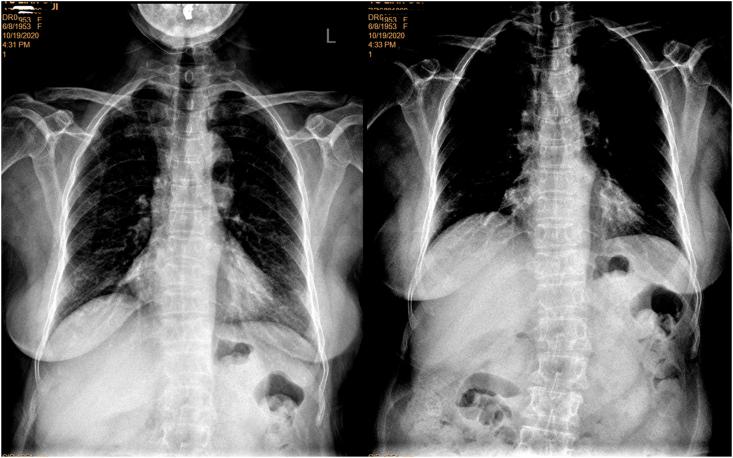
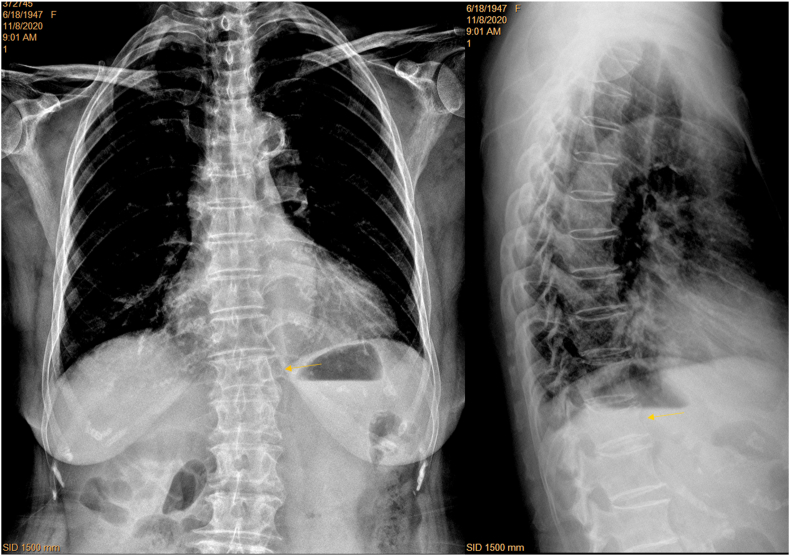
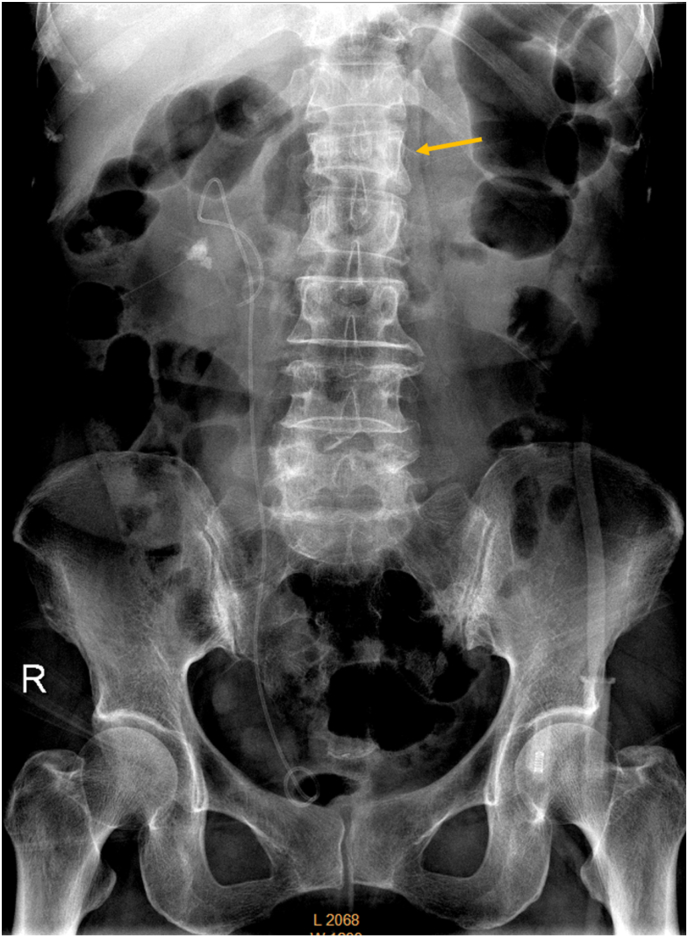
For standardly filmed CFR, spine readability was similar among those from Hospitals-A, B, and C, while performed less well for those from Hospital-D. With the prospective cases from Hospitals-A and B, spines readable to vertebra L1 level or lower increased from 48.2% for standard filming to 80.7% for adjusted filming. Spines with 'blurry' labelling decreased from 35.7% for standard filming to 15.7% for adjusted filming. For the 84 prospective cases, 42.9% (36/84) of the patients had OVF, and 26 cases of CLR positive cases were detected as having vertebral deformity on CFR. For minimal OVF cases (<20% height loss), 38% (5/13) were detected on CFR. Among 22 cases with apparent OVF (≥20% height loss), two cases were missed on CFR. False positivity was labelled in five cases, among them four cases had 'burry' spines.
CFR can help opportunistically detect OVF, which can be further improved if X-ray beam is adjusted to towards vertebra T8 instead of towards vertebra T6.
This study confirms that CFR can help detect OVF opportunistically, and the visibility of the mid/lower thoracic spine and thoracolumbar junction can be much improved after minor adjustment of X-ray beam positioning. This study also suggests high positive rate of OVF in elderly Chinese female patients indicated for chest radiograph. Radiologists should be trained and sensitized in vertebral deformity identification on CFR as the clinical management can be improved by opportunistic detection of OVF.
在临床上,胸部正位X线片(CFR)常用于疑似患有呼吸系统疾病的患者以及用于评估心脏和大血管。CFR可用于机会性地检测骨质疏松性椎体骨折(OVF)。然而,对于标准的CFR,OVF患病率最高的部位,即胸腰段交界处,通常偏离X线束焦点。本研究检验了这样一个假设,即如果CFR拍摄时比标准X线束定位低大约两个椎体,胸腰段交界处的可视化效果会有很大改善。
四家医院(A、B、C、D)提供了101例老年女性的数字化CFR,采用标准拍摄(分别为28例、20例、24例和21例)。从A医院和B医院前瞻性招募了84例老年女性患者,她们是因脊柱疾病以外的指征而被转诊进行胸部X线检查的连续患者。对于这些前瞻性CFR,将X线束焦点从T6椎体调整至T8椎体,并获得标准侧位X线片作为参考。在CFR上评估脊柱的可见性和OVF的可检测性。在排除其他影像学和临床潜在病因后,根据胸部侧位X线片(CLR)诊断OVF。
对于标准拍摄的CFR,A、B和C医院的脊柱可读性相似,而D医院的表现较差。对于A医院和B医院的前瞻性病例,可读到L1椎体及以下的脊柱从标准拍摄时的48.2%增加到调整拍摄时的80.7%。标记“模糊”的脊柱从标准拍摄时的35.7%降至调整拍摄时的15.7%。对于84例前瞻性病例,42.9%(36/84)的患者患有OVF,26例CLR阳性病例在CFR上被检测出有椎体畸形。对于轻度OVF病例(椎体高度丢失<20%),38%(5/13)在CFR上被检测出。在22例明显OVF病例(椎体高度丢失≥20%)中,有2例在CFR上漏诊。有5例假阳性标记,其中4例脊柱“模糊”。
CFR有助于机会性地检测OVF,如果将X线束调整至T8椎体而不是T6椎体,检测效果可进一步提高。
本研究证实CFR有助于机会性地检测OVF,对X线束定位进行微小调整后,胸段中下部脊柱和胸腰段交界处的可视化效果可得到很大改善。本研究还提示,因胸部X线检查而就诊的中国老年女性患者中OVF的阳性率较高。放射科医生应接受培训并提高在CFR上识别椎体畸形的意识,因为机会性检测OVF可改善临床管理。