Douin David J, Anderson Erin L, Dylla Layne, Rice John D, Jackson Conner L, Wright Franklin L, Bebarta Vikhyat S, Schauer Steven G, Ginde Adit A
Department of Anesthesiology, University of Colorado School of Medicine, Aurora, CO.
Department of Emergency Medicine, University of Colorado School of Medicine, Aurora, CO.
Crit Care Explor. 2021 May 14;3(5):e0418. doi: 10.1097/CCE.0000000000000418. eCollection 2021 May.
Hyperoxia is common among critically ill patients and may increase morbidity and mortality. However, limited evidence exists for critically injured patients. The objective of this study was to determine the association between hyperoxia and in-hospital mortality in adult trauma patients requiring ICU admission.
This multicenter, retrospective cohort study was conducted at two level I trauma centers and one level II trauma center in CO between October 2015 and June 2018. All adult trauma patients requiring ICU admission within 24 hours of emergency department arrival were eligible. The primary exposure was oxygenation during the first 7 days of hospitalization.
None.
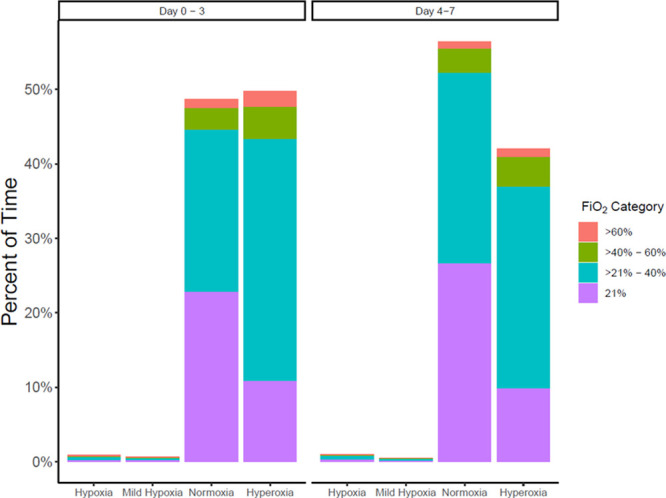
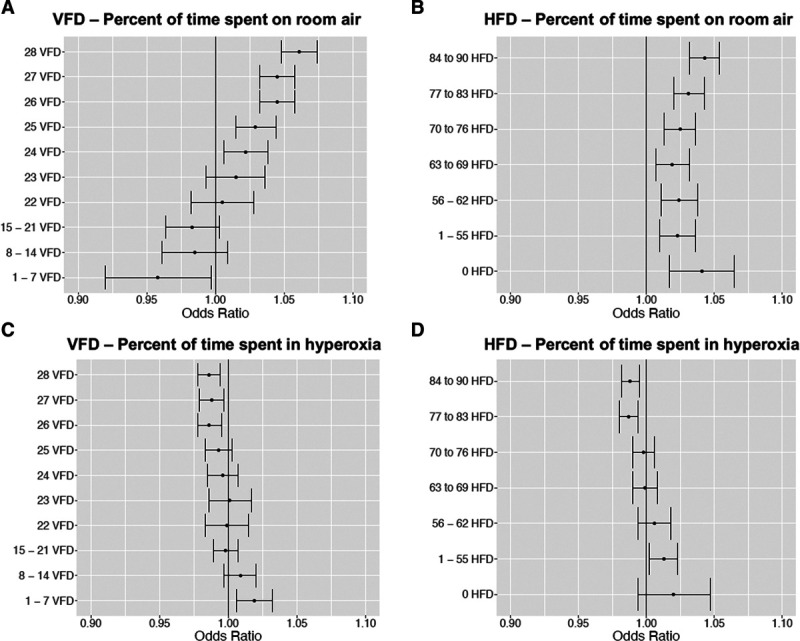
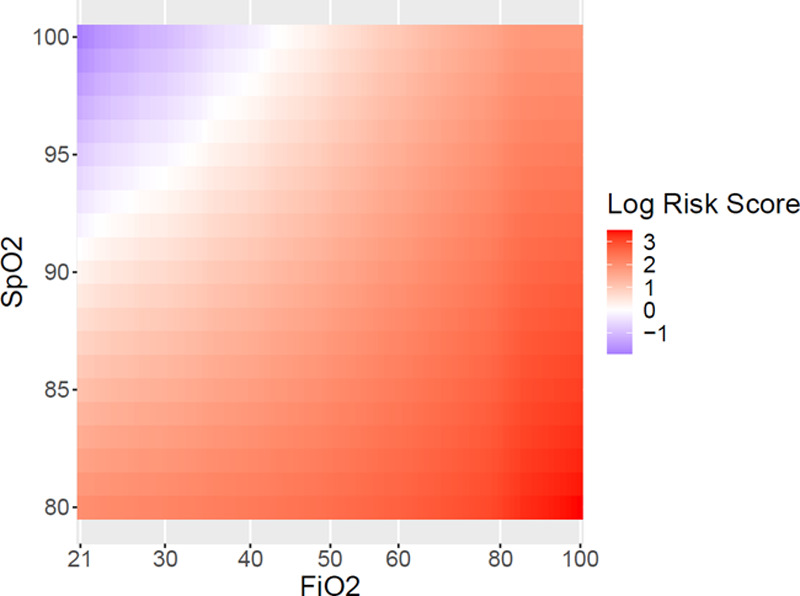
Primary outcome was in-hospital mortality. Secondary outcomes were hospital-free days and ventilator-free days. We included 3,464 critically injured patients with a mean age of 52.6 years. Sixty-five percent were male, and 66% had blunt trauma mechanism of injury. The primary outcome of in-hospital mortality occurred in 264 patients (7.6%). Of 226,057 patient-hours, 46% were spent in hyperoxia (oxygen saturation > 96%) and 52% in normoxia (oxygen saturation 90-96%). During periods of hyperoxia, the adjusted risk for mortality was higher with greater oxygen administration. At oxygen saturation of 100%, the adjusted risk scores for mortality (95% CI) at Fio of 100%, 80%, 60%, and 50% were 6.4 (3.5-11.8), 5.4 (3.4-8.6), 2.7 (1.7-4.1), and 1.5 (1.1-2.2), respectively. At oxygen saturation of 98%, the adjusted risk scores for mortality (95% CI) at Fio of 100%, 80%, 60%, and 50% were 7.7 (4.3-13.5), 6.3 (4.1-9.7), 3.2 (2.2-4.8), and 1.9 (1.4-2.7), respectively.
During hyperoxia, higher oxygen administration was independently associated with a greater risk of mortality among critically injured patients. Level of evidence: Cohort study, level III.
高氧血症在重症患者中很常见,可能会增加发病率和死亡率。然而,针对严重受伤患者的证据有限。本研究的目的是确定需要入住重症监护病房(ICU)的成年创伤患者中高氧血症与院内死亡率之间的关联。
设计、地点和参与者:这项多中心回顾性队列研究于2015年10月至2018年6月在科罗拉多州的两个一级创伤中心和一个二级创伤中心进行。所有在急诊科就诊后24小时内需要入住ICU的成年创伤患者均符合条件。主要暴露因素是住院前7天的氧合情况。
无。
主要结局是院内死亡率。次要结局是无住院天数和无呼吸机天数。我们纳入了3464例严重受伤患者,平均年龄为52.6岁。65%为男性,66%有钝性创伤机制。264例患者(7.6%)发生了院内死亡这一主要结局。在226057个患者小时中,46%的时间处于高氧血症(氧饱和度>96%),52%的时间处于正常氧合(氧饱和度90 - 96%)。在高氧血症期间,氧输送量越高,校正后的死亡风险越高。在氧饱和度为100%时,吸入氧分数(FiO₂)为100%、80%、60%和50%时的校正死亡风险评分(95%置信区间)分别为6.4(3.5 - 11.8)、5.4(3.4 - 8.6)、2.7(1.7 - 4.1)和1.5(1.1 - 2.2)。在氧饱和度为98%时,FiO₂为100%、80%、60%和50%时的校正死亡风险评分(95%置信区间)分别为7.7(4.3 - 13.5)、6.3(4.1 - 9.7)、3.2(2.2 - 4.8)和1.9(1.4 - 2.7)。
在高氧血症期间,较高的氧输送量与严重受伤患者更高的死亡风险独立相关。证据级别:队列研究,III级。