Division of Rheumatology, Hopital Maison Blanche, Reims, France.
Department of Internal Medicine and Clinical Immunlogy, Sorbonne Université, Pitié-Salpêtrière University Hospital, Paris, France.
Brain Pathol. 2021 May;31(3):e12955. doi: 10.1111/bpa.12955.
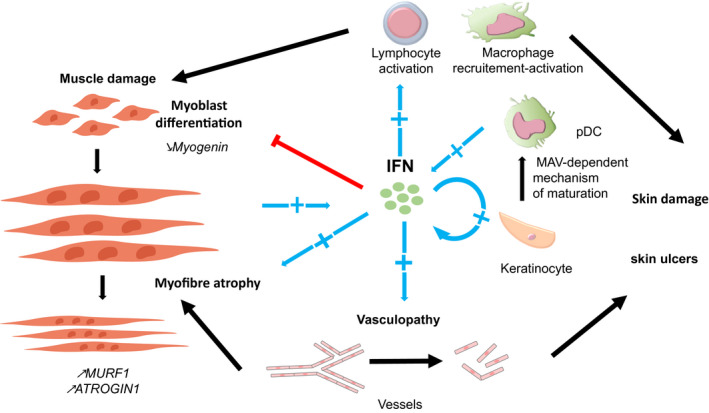
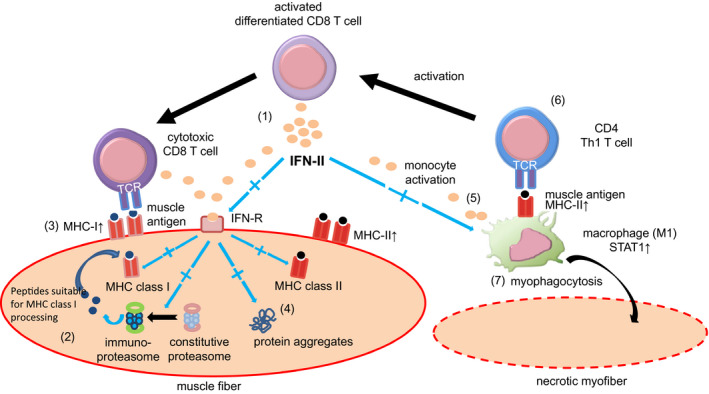
The classification of idiopathic inflammatory myopathies (IIM) is based on clinical, serological and histological criteria. The identification of myositis-specific antibodies has helped to define more homogeneous groups of myositis into four dominant subsets: dermatomyositis (DM), antisynthetase syndrome (ASyS), sporadic inclusion body myositis (sIBM) and immune-mediated necrotising myopathy (IMNM). sIBM and IMNM patients present predominantly with muscle involvement, whereas DM and ASyS patients present additionally with other extramuscular features, such as skin, lung and joints manifestations. Moreover, the pathophysiological mechanisms are distinct between each myositis subsets. Recently, interferon (IFN) pathways have been identified as key players implicated in the pathophysiology of myositis. In DM, the key role of IFN, especially type I IFN, has been supported by the identification of an IFN signature in muscle, blood and skin of DM patients. In addition, DM-specific antibodies are targeting antigens involved in the IFN signalling pathways. The pathogenicity of type I IFN has been demonstrated by the identification of mutations in the IFN pathways leading to genetic diseases, the monogenic interferonopathies. This constitutive activation of IFN signalling pathways induces systemic manifestations such as interstitial lung disease, myositis and skin rashes. Since DM patients share similar features in the context of an acquired activation of the IFN signalling pathways, we may extend underlying concepts of monogenic diseases to acquired interferonopathy such as DM. Conversely, in ASyS, available data suggest a role of type II IFN in blood, muscle and lung. Indeed, transcriptomic analyses highlighted a type II IFN gene expression in ASyS muscle tissue. In sIBM, type II IFN appears to be an important cytokine involved in muscle inflammation mechanisms and potentially linked to myodegenerative features. For IMNM, currently published data are scarce, suggesting a minor implication of type II IFN. This review highlights the involvement of different IFN subtypes and their specific molecular mechanisms in each myositis subset.
特发性炎性肌病(IIM)的分类基于临床、血清学和组织学标准。肌炎特异性抗体的鉴定有助于将更为同质的肌炎组分为四个主要亚型:皮肌炎(DM)、抗合成酶综合征(ASyS)、散发性包涵体肌炎(sIBM)和免疫介导的坏死性肌病(IMNM)。sIBM 和 IMNM 患者主要表现为肌肉受累,而 DM 和 ASyS 患者除肌肉外还表现出其他肌肉外特征,如皮肤、肺和关节表现。此外,每种肌炎亚型的病理生理机制均不同。最近,干扰素(IFN)途径已被确定为参与肌炎病理生理学的关键因素。在 DM 中,IFN,特别是 I 型 IFN 的关键作用得到了 DM 患者肌肉、血液和皮肤中 IFN 特征的支持。此外,DM 特异性抗体针对涉及 IFN 信号通路的抗原。IFN 信号通路的突变导致遗传疾病,即单基因干扰素病,鉴定出了 I 型 IFN 的致病性。这种 IFN 信号通路的组成性激活诱导了间质性肺病、肌炎和皮疹等全身表现。由于 DM 患者在获得性 IFN 信号通路激活的背景下具有相似的特征,我们可以将单基因疾病的潜在概念扩展到获得性干扰素病,如 DM。相反,在 ASyS 中,现有数据表明 II 型 IFN 在血液、肌肉和肺部中发挥作用。实际上,转录组分析突出了 ASyS 肌肉组织中 II 型 IFN 的基因表达。在 sIBM 中,II 型 IFN 似乎是一种参与肌肉炎症机制的重要细胞因子,并且可能与肌退行性特征相关。对于 IMNM,目前发表的数据很少,表明 II 型 IFN 的影响较小。本综述强调了不同 IFN 亚型及其在每种肌炎亚型中的特定分子机制的参与。