Ha Eun Ju, Shin Jung Hee, Na Dong Gyu, Jung So Lyung, Lee Young Hen, Paik Wooyul, Hong Min Ji, Kim Yeo Koon, Lee Chang Yoon
Department of Radiology, Ajou University School of Medicine, Suwon, Korea.
Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Ultrasonography. 2021 Oct;40(4):594-601. doi: 10.14366/usg.21056. Epub 2021 Apr 5.
This study compared the diagnostic performance of the modified Korean Thyroid Imaging Reporting and Data System (K-TIRADS) for thyroid malignancy with three international guidelines.
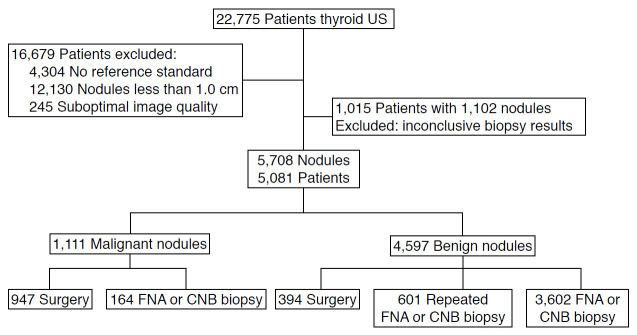
From June to September 2015, 5,708 thyroid nodules (≥1.0 cm) in 5,081 consecutive patients who underwent thyroid ultrasound (US) at 26 institutions were evaluated. The US features of the thyroid nodules were retrospectively reviewed and classified according to all four guidelines. In the modified K-TIRADS, the biopsy size threshold was changed to 2.0 cm for K-TIRADS 3 and 1.0 or 1.5 cm for K-TIRADS 4 (K-TIRADS1.0cm and K-TIRADS1.5cm, respectively). We compared the diagnostic performance and unnecessary fine-needle aspiration biopsy (FNAB) rates for thyroid malignancy between the modified K-TIRADS and three international guidelines.
Of the 5,708 thyroid nodules, 4,597 (80.5%) were benign and 1,111 (19.5%) were malignant. The overall sensitivity was highest for the modified K-TIRADS1.0cm (91.0%), followed by the European (EU)-TIRADS (84.6%), American Association of Clinical Endocrinologists/American College of Endocrinology/Associazione Medici Endocrinologi (AACE/ACE/AME) (80.5%), American College of Radiology (ACR)-TIRADS (76.1%), and modified K-TIRADS1.5cm (76.1%). For large nodules (>2.0 cm), the sensitivity increased to 98.0% in both the modified K-TIRADS1.0cm and K-TIRADS1.5cm. For small nodules (≤2.0 cm), the unnecessary FNAB rate was lowest with the modified K-TIRADS1.5cm (17.6%), followed by the ACR-TIRADS (18.6%), AACE/ACE/AME (19.3%), EU-TIRADS (28.1%), and modified K-TIRADS1.0cm (31.2%).
The modified K-TIRADS1.5cm can reduce the unnecessary FNAB rate for small nodules (1.0-2.0 cm), while maintaining high sensitivity for detecting malignancies >2.0 cm.
本研究比较了改良的韩国甲状腺影像报告和数据系统(K-TIRADS)对甲状腺恶性肿瘤的诊断性能与三项国际指南。
2015年6月至9月,对26家机构连续5081例接受甲状腺超声(US)检查的患者中的5708个甲状腺结节(≥1.0 cm)进行了评估。回顾性分析甲状腺结节的超声特征,并根据所有四项指南进行分类。在改良的K-TIRADS中,K-TIRADS 3类的活检大小阈值改为2.0 cm,K-TIRADS 4类的活检大小阈值改为1.0 cm或1.5 cm(分别为K-TIRADS1.0cm和K-TIRADS1.5cm)。我们比较了改良的K-TIRADS与三项国际指南对甲状腺恶性肿瘤的诊断性能和不必要的细针穿刺活检(FNAB)率。
在5708个甲状腺结节中,4597个(80.5%)为良性,1111个(19.5%)为恶性。改良的K-TIRADS1.0cm的总体敏感性最高(91.0%),其次是欧洲(EU)-TIRADS(84.6%)、美国临床内分泌学家协会/美国内分泌学会/意大利内分泌医生协会(AACE/ACE/AME)(80.5%)、美国放射学会(ACR)-TIRADS(76.1%)和改良的K-TIRADS-1.5cm(76.1%)。对于大结节(>2.0 cm),改良的K-TIRADS1.0cm和K-TIRADS1.5cm的敏感性均提高到98.0%。对于小结节(≤2.0 cm),改良的K-TIRADS1.5cm的不必要FNAB率最低(17.6%),其次是ACR-TIRADS(18.6%)、AACE/ACE/AME(19.3%)、EU-TIRADS(28.1%)和改良的K-TIRADS1.0cm(31.2%)。
改良的K-TIRADS1.5cm可以降低小结节(1.0~2.0 cm)的不必要FNAB率,同时保持对>2.0 cm恶性肿瘤的高敏感性。