Kim Young-Hoon, Kang Ho, Dho Yun-Sik, Hwang Kihwan, Joo Jin-Deok, Kim Yong Hwy
Department of Neurological Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Department of Neurosurgery, Seoul National University Hospital, Seoul, Korea.
J Korean Neurosurg Soc. 2021 Jul;64(4):619-630. doi: 10.3340/jkns.2020.0231. Epub 2021 May 28.
The skull base reconstruction step, which prevents cerebrospinal fluid (CSF) leakage, is one of the most challenging steps in endoscopic skull base surgery (ESS). The purpose of this study was to assess the outcomes and complications of a reconstruction technique for immediate CSF leakage repair using multiple onlay grafts following ESS.
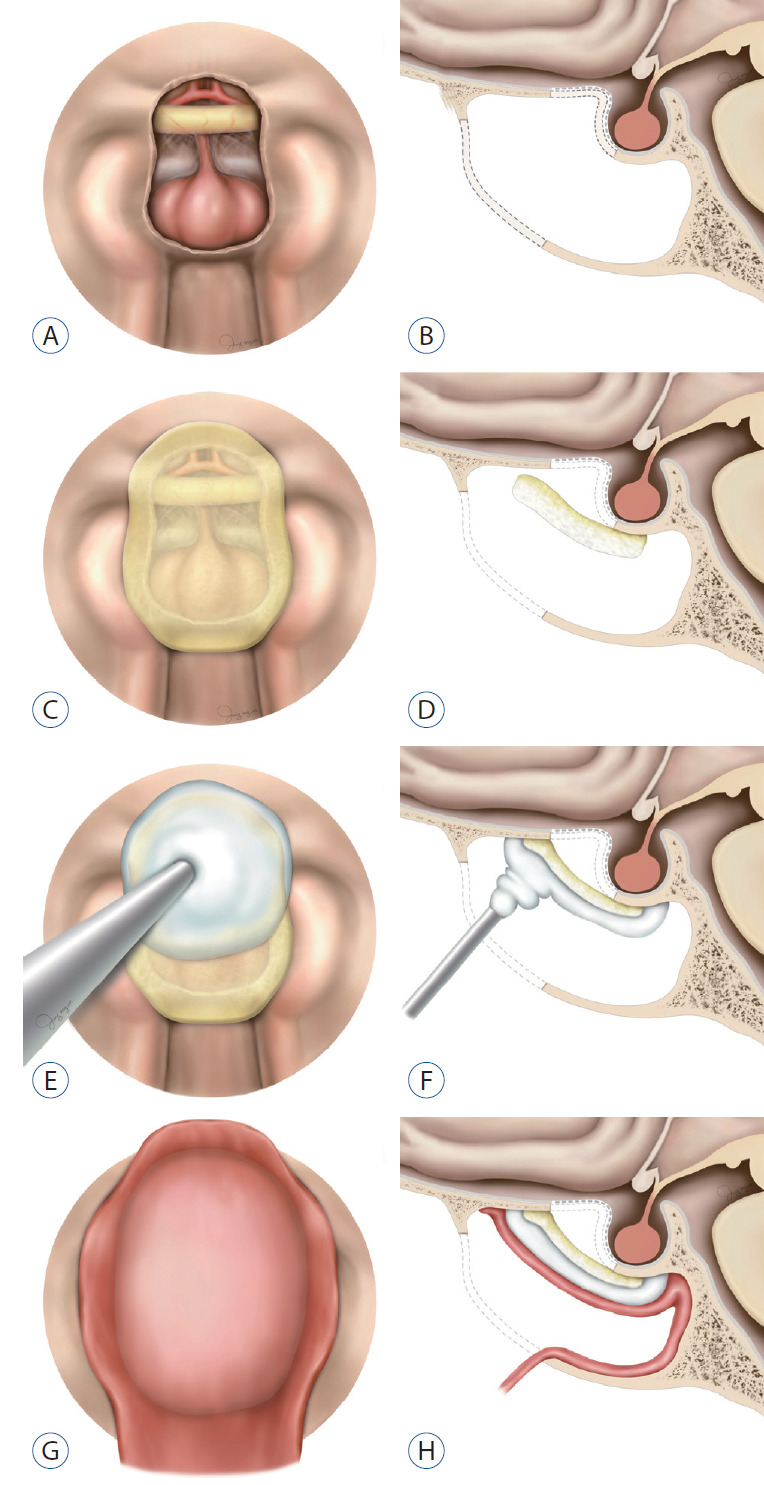
A total of 230 consecutive patients who underwent skull base reconstruction using multiple onlay grafts with fibrin sealant patch (FSP), hydroxyapatite cement (HAC), and pedicled nasoseptal flap (PNF) for high-flow CSF leakage following ESS at three institutions were enrolled. We retrospectively reviewed the medical and radiological records to analyze the preoperative features and postoperative results.
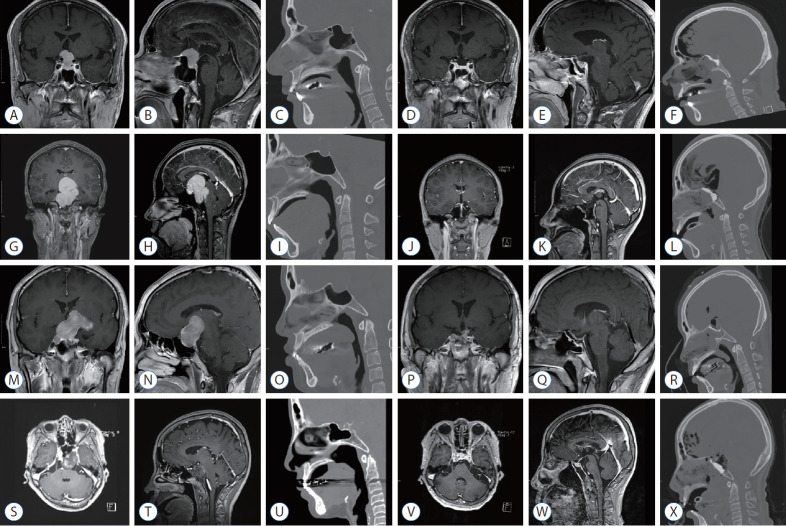
The diagnoses included craniopharyngioma (46.8%), meningioma (34.0%), pituitary adenoma (5.3%), chordoma (1.6%), Rathke's cleft cyst (1.1%) and others (n=21, 11.2%). The trans-planum/tuberculum approach (94.3%) was the most commonly adapted surgical method, followed by the trans-sellar and transclival approaches. The third ventricle was opened in 78 patients (41.5%). Lumbar CSF drainage was not performed postoperatively in any of the patients. Postoperative CSF leakage occurred in four patients (1.7%) due to technical mistakes and were repaired with the same technique. However, postoperative meningitis occurred in 13.5% (n=31) of the patients, but no microorganisms were identified. The median latency to the diagnosis of meningitis was 8 days (range, 2-38). CSF leakage was the unique risk factor for postoperative meningitis (p<0.001).
The use of multiple onlay grafts with FSP, HAC, and PNF is a reliable reconstruction technique that provides immediate and complete CSF leakage repair and mucosal grafting on the skull base without the need to harvest autologous tissue or perform postoperative CSF diversion. However, postoperative meningitis should be monitored carefully.
颅底重建步骤是预防脑脊液(CSF)漏出的关键环节,也是内镜颅底手术(ESS)中最具挑战性的步骤之一。本研究旨在评估ESS术后使用多种覆盖移植物进行即时CSF漏修补的重建技术的疗效及并发症。
共有230例连续患者在三个机构接受了ESS术后使用纤维蛋白密封剂贴片(FSP)、羟基磷灰石水泥(HAC)和带蒂鼻中隔瓣(PNF)进行多种覆盖移植物的颅底重建,以修复高流量CSF漏。我们回顾性分析了医疗和放射学记录,以分析术前特征和术后结果。
诊断包括颅咽管瘤(46.8%)、脑膜瘤(34.0%)、垂体腺瘤(5.3%)、脊索瘤(1.6%)、拉克氏囊肿(1.1%)和其他(n=21,11.2%)。经蝶鞍/结节入路(94.3%)是最常用的手术方法,其次是经鞍和经斜坡入路。78例患者(41.5%)打开了第三脑室。所有患者术后均未进行腰大池脑脊液引流。4例患者(1.7%)因技术失误发生术后CSF漏,并采用相同技术进行了修复。然而,13.5%(n=31)的患者发生了术后脑膜炎,但未发现微生物。脑膜炎诊断的中位潜伏期为8天(范围2-38天)。CSF漏是术后脑膜炎的唯一危险因素(p<0.001)。
使用FSP、HAC和PNF的多种覆盖移植物是一种可靠的重建技术,可即时、完全修复CSF漏,并在颅底进行黏膜移植,无需采集自体组织或进行术后CSF分流。然而,术后应密切监测脑膜炎。