Division of Thoracic Oncology, Shizuoka Cancer Center, 1007 Shimonagakubo, Nagaizumi, Sunto-gun, Shizuoka, 411-8777, Japan.
Division of Gastrointestinal Oncology, Shizuoka Cancer Center, 1007 Shimonagakubo, Nagaizumi, Sunto-gun, Shizuoka, 411-8777, Japan.
Invest New Drugs. 2021 Dec;39(6):1716-1723. doi: 10.1007/s10637-021-01136-z. Epub 2021 May 28.
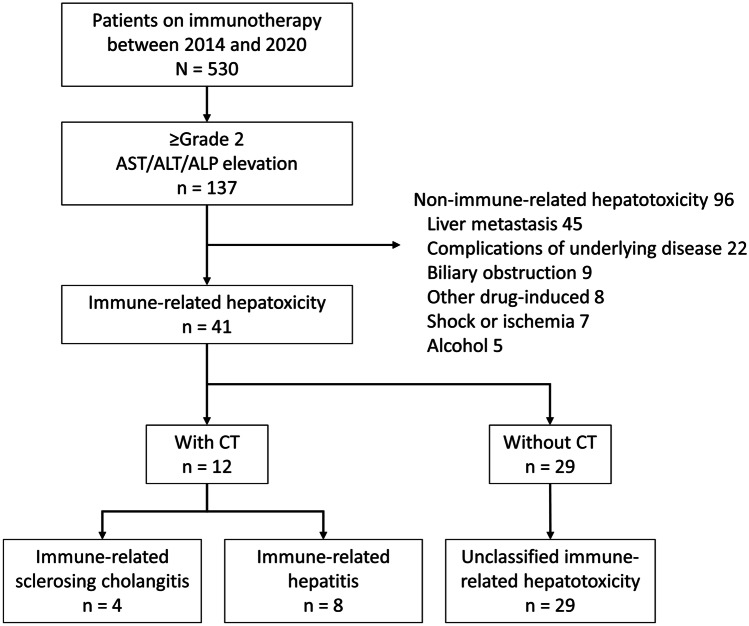
Background Immune-related hepatotoxicity is often regarded as immune-related hepatitis (irHepatitis) despite including immune-related sclerosing cholangitis (irSC). This study examined the clinical differences between irSC and irHepatitis. Methods A single-center retrospective study of 530 consecutive patients who received immunotherapy between August 2014 and April 2020 was performed. IrSC and irHepatitis were respectively defined as the radiological presence and absence of bile duct dilation and wall thickness. Results Forty-one patients (7.7%) developed immune-related hepatotoxicity. A CT scan was performed on 12 patients, including 11 of 12 with ≥ grade 3 aminotransferase elevations. IrSC and irHepatitis were diagnosed in 4 (0.8%) and 8 (1.5%) patients, respectively. All the irSC patients had been treated with anti-PD-1. IrHepatitis was more common among patients receiving anti-CTLA-4 than among those receiving anti-PD-1/PD-L1 inhibitors (14%, 7/50 vs. 0.2%, 1/480, P < 0.001). A ≥ grade 2 alkaline phosphatase (ALP) elevation resulting in a cholestatic pattern was seen in all 4 irSC patients. Among the irSC patients, 3 (3/4, 75%) developed ≥ grade 3 aminotransferases elevation. The median duration from the start of immunotherapy until ≥ grade 2 liver enzymes elevation was 257 and 55.5 days in irSC and irHepatitis patients. The median times for progression from grade 2 to 3 liver enzyme elevation were 17.5 and 0 days, respectively. Conclusions IrSC and irHepatitis have different characteristics in the class of immune checkpoint inhibitor and onset pattern. Radiological examination for the diagnosis of irSC should be considered for patients with ≥ grade 2 ALP elevation resulting in a cholestatic pattern. (Registration number J2020-36, Date of registration June 3, 2020).
背景 免疫相关性肝毒性通常被认为是免疫性肝炎(irHepatitis),尽管它包括免疫性硬化性胆管炎(irSC)。本研究旨在探讨 irSC 和 irHepatitis 之间的临床差异。
方法 对 2014 年 8 月至 2020 年 4 月期间接受免疫治疗的 530 例连续患者进行了单中心回顾性研究。irSC 和 irHepatitis 分别定义为胆管扩张和胆管壁增厚的影像学存在和不存在。
结果 41 例(7.7%)患者发生免疫相关性肝毒性。对 12 例患者进行了 CT 扫描,其中 12 例中有 11 例转氨酶升高≥3 级。分别诊断出 4 例(0.8%)和 8 例(1.5%)irSC 和 irHepatitis 患者。所有 irSC 患者均接受了抗 PD-1 治疗。接受抗 CTLA-4 治疗的患者比接受抗 PD-1/PD-L1 抑制剂治疗的患者更易发生 irHepatitis(14%,7/50 比 0.2%,1/480,P<0.001)。4 例 irSC 患者均出现碱性磷酸酶(ALP)升高≥2 级,表现为胆汁淤积型。在 irSC 患者中,有 3 例(3/4,75%)出现转氨酶升高≥3 级。免疫治疗开始至出现≥2 级肝酶升高的中位时间分别为 irSC 和 irHepatitis 患者的 257 和 55.5 天。从 2 级进展到 3 级肝酶升高的中位时间分别为 17.5 和 0 天。
结论 在免疫检查点抑制剂的类别和发病模式上,irSC 和 irHepatitis 具有不同的特征。对于出现 ALP 升高≥2 级且呈胆汁淤积型的患者,应考虑进行影像学检查以明确 irSC 的诊断。(注册号 J2020-36,注册日期 2020 年 6 月 3 日)。