Department of Physiology and Biophysics & Center for Proteomics and Molecular Therapeutics, The Chicago Medical School, Rosalind Franklin University, North Chicago, IL, United States.
Med Hypotheses. 2021 Jul;152:110609. doi: 10.1016/j.mehy.2021.110609. Epub 2021 May 12.
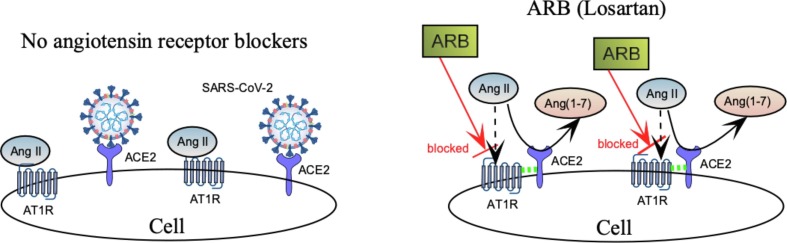
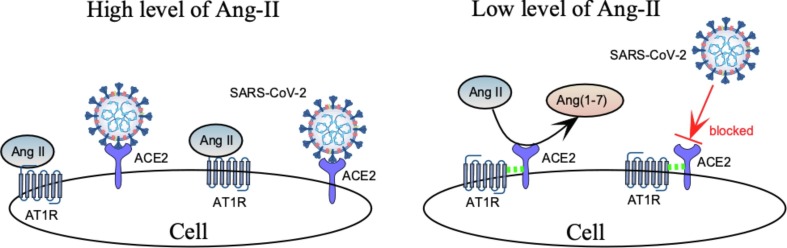
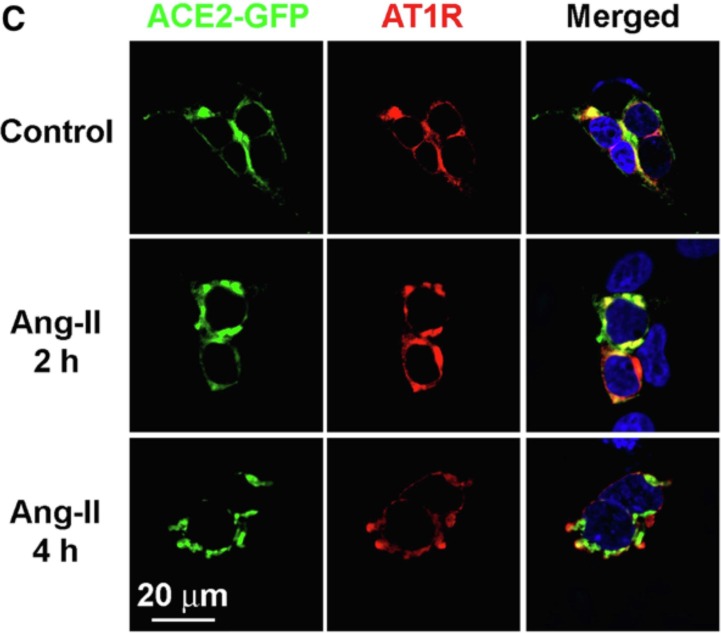
Preexisting hypertension is a known risk factor for severe COVID-19. Abnormal activation of RAS upregulates angiotensin II (Ang-II) and contributes to severe manifestations of COVID-19. Although RAS inhibitors (RASi) are a mainstay of antihypertensive therapy, they have been associated (in some animal studies) with an increase in angiotensin converting enzyme 2 (ACE2) receptors that facilitate cellular entry of the SARS-CoV-2 virus. Nonetheless, current medical practice does not recommend curtailing RASi to protect hypertensive patients from COVID. On the contrary, there is clinical evidence to support a beneficial effect of RASi for hypertensive patients in the midst of a COVID-19 pandemic, although the precise mechanism for this is unclear. In this paper, we hypothesize that RASi reduces the severity of COVID-19 by promoting ACE2-AT1R complex formation at the cell surface, where AT1R mediates the major vasopressor effects of Ang-II. Furthermore, we propose that the interaction between ACE2 and AT1R impedes binding of SARS-CoV-2 to ACE2, thereby allowing ACE2 to convert Ang-II to the more beneficial Ang(1-7), that has vasodilator and anti-inflammatory activity. Evidence for ACE2-AT1R complex formation during reduced Ang-II comes from receptor colocalization studies in isolated HEK293 cells, but this has not been confirmed in cells having endogenous expression of ACE2 and AT1R. Since the SARS-CoV-2 virus attacks the kidney, as well as the heart and lung, our hypothesis for the effect of RASi on COVID-19 could be tested in vitro using human proximal tubule cells (HK-2), having ACE2 and AT1 receptors. Specifically, colocalization of fluorescent labelled: SARS-CoV-2 spike protein, ACE2, and AT1R in HK-2 cells can be used to clarify the mechanism of RASi action in renal and lung epithelia, which could lead to protocols for reducing the severity of COVID-19 in both hypertensive and normotensive patients.
先前存在的高血压是 COVID-19 重症的已知危险因素。RAS 的异常激活会上调血管紧张素 II(Ang-II),并导致 COVID-19 的严重表现。尽管 RAS 抑制剂(RASi)是抗高血压治疗的主要药物,但它们与增加血管紧张素转化酶 2(ACE2)受体有关,这有助于 SARS-CoV-2 病毒进入细胞。尽管如此,目前的医疗实践并不建议为了保护高血压患者免受 COVID 的影响而停止使用 RASi。相反,有临床证据支持 RASi 对 COVID-19 大流行期间的高血压患者有益,尽管其确切机制尚不清楚。在本文中,我们假设 RASi 通过促进细胞表面 ACE2-AT1R 复合物的形成来减轻 COVID-19 的严重程度,其中 AT1R 介导 Ang-II 的主要血管加压作用。此外,我们提出 ACE2 和 AT1R 之间的相互作用会阻碍 SARS-CoV-2 与 ACE2 的结合,从而使 ACE2 将 Ang-II 转化为更有益的 Ang(1-7),后者具有血管扩张和抗炎作用。在 Ang-II 减少时 ACE2-AT1R 复合物形成的证据来自于在分离的 HEK293 细胞中进行的受体共定位研究,但这在具有内源性表达 ACE2 和 AT1R 的细胞中尚未得到证实。由于 SARS-CoV-2 病毒攻击肾脏以及心脏和肺部,我们对 RASi 对 COVID-19 影响的假设可以在体外使用具有 ACE2 和 AT1 受体的人近端肾小管细胞 (HK-2) 进行测试。具体来说,可以使用共定位荧光标记的 SARS-CoV-2 刺突蛋白、ACE2 和 AT1R 来澄清 RASi 在肾和肺上皮细胞中的作用机制,这可能会导致减少高血压和正常血压患者 COVID-19 严重程度的方案。