School of Medical Sciences, Faculty of Medicine and Health, Örebro University, Örebro, Sweden.
Department of Orthopedics, Faculty of Medicine and Health, Örebro University, Örebro, Sweden.
Clin Orthop Relat Res. 2021 Oct 1;479(10):2203-2213. doi: 10.1097/CORR.0000000000001838.
Prosthetic joint infection (PJI) is a complication after arthroplasty that negatively affects patient health. However, prior reports have not addressed the long-term consequences of hip PJI in terms of patient mortality, quality of life, and hip function.
QUESTIONS/PURPOSES: At a minimum of 10 years after PJI in patients undergoing primary THA, in the context of several large, national databases in Sweden, we asked: (1) Is mortality increased for patients with PJI after THA compared with patients with a noninfected THA? (2) Does PJI of the hip have a negative influence on quality of life as measured by the Euro-QoL-5D-5L (EQ-5D-5L), ambulatory aids, residential status, and hip function as measured by the Oxford Hip Score (OHS)? (3) Which factors are associated with poor patient-reported outcome measures (PROMs) for patients with PJI after primary THA?
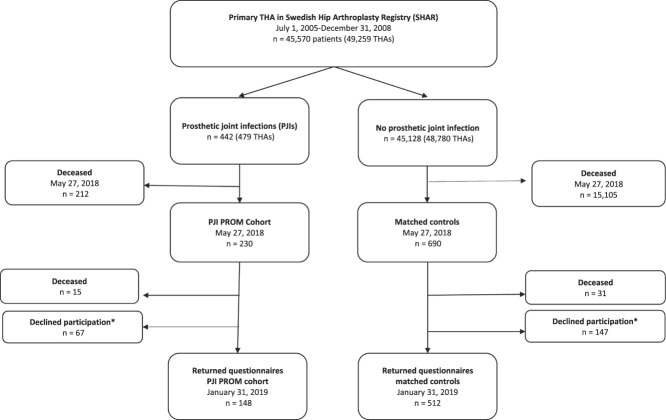
This study included 442 patients with a PJI after primary THA, from a previously published national study, including all patients with a THA performed from 2005 to 2008 in Sweden (n = 45,570) recruited from the Swedish Hip Arthroplasty Registry (SHAR). Possible deep PJIs were identified in the Swedish Dispensed Drug Registry and verified by review of medical records. Mortality in patients with PJI was compared with the remaining cohort of 45,128 patients undergoing primary THA who did not have PJI. Mortality data were retrieved from the SHAR, which in turn is updated daily from the population registry. A subgroup analysis of patients who underwent primary THA in 2008 was performed to adjust for the effect of comorbidities on mortality, as American Society of Anesthesiologists (ASA) scores became available in the SHAR at that time. For the PROM analysis, we identified three controls matched by age, gender, indication for surgery, and year of operation to each living PJI patient. A questionnaire including EQ-5D-5L, ambulatory aids, residential status, and OHS was collected from patients with PJI and controls at a mean of 11 years from the primary procedure. Apart from age and gender, we analyzed reoperation data (such as number of reoperations and surgical approach) and final prosthesis in situ to explore possible factors associated with poor PROM results.
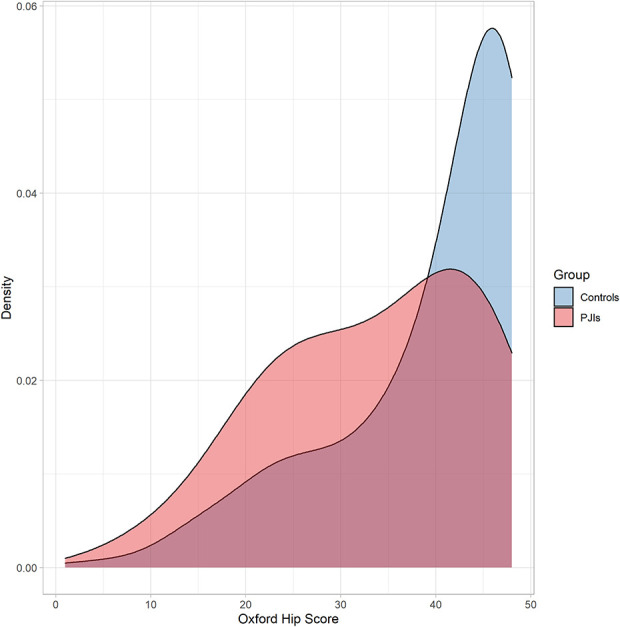
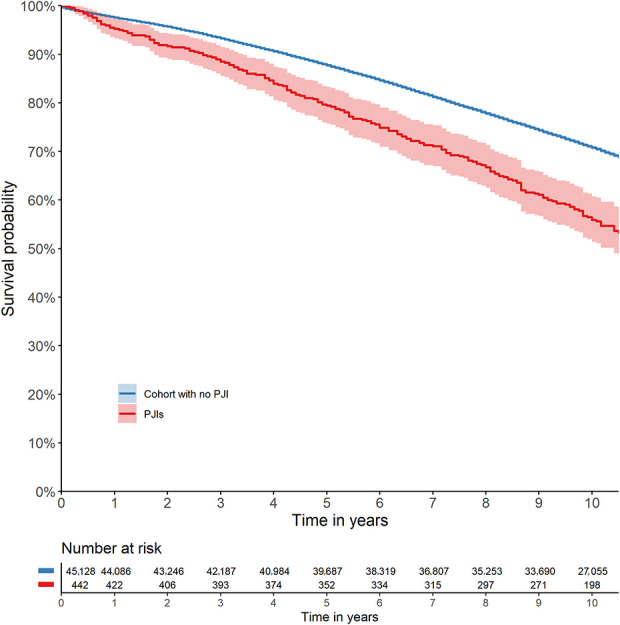
After controlling for differences in sex, age, and indication for surgery, we found the all-cause 10-year mortality higher for patients with PJI (45%) compared with patients undergoing THA without PJI (29%) (odds ratio 1.4 [95% CI 1.2 to 1.6]; p < 0.001). The questionnaire, with a minimum of 10 years of follow-up, revealed a lower EQ-5D-5L index score (0.83 versus 0.94, -0.13 [95% CI -0.18 to -0.08; p < 0.001]), greater proportion of assisted living (21% versus 12%, OR 2.0 [95% CI 1.2 to 3.3]; p = 0.01), greater need of ambulatory aids (65% versus 42%, OR 3.1 [95% 2.1 to 4.8]; p < 0.001), and a lower OHS score (36 versus 44, -5.9 [-7.7 to -4.0]; p < 0.001) for patients with PJI than for matched controls. Factors associated with lower OHS score for patients with PJI were three or more reoperations (-8.0 [95% CI -13.0 to -3.2]; p = 0.01) and a direct lateral approach used at revision surgery compared with a posterior approach (-4.3 [95% CI -7.7 to -0.9]; p = 0.01).
In this study, we found that PJI after THA has a negative impact on mortality, long-term health-related quality of life, and hip function. Furthermore, the subgroup analysis showed that modifiable factors such as the number of reoperations and surgical approach are associated with poorer hip function. This emphasizes the importance of prompt, proper initial treatment to reduce repeated surgery to minimize the negative long-term effects of hip PJI.
Level III, therapeutic study.
人工关节感染(PJI)是关节置换术后的一种并发症,会对患者的健康产生负面影响。然而,之前的报告并未涉及髋关节 PJI 对患者死亡率、生活质量和髋关节功能的长期影响。
问题/目的:在瑞典的几个大型国家数据库中,对接受初次全髋关节置换术(THA)后发生髋关节 PJI 的患者进行至少 10 年的随访,我们提出了以下问题:(1)与未感染的 THA 患者相比,THA 后发生 PJI 的患者死亡率是否增加?(2)髋关节 PJI 是否会对生活质量(通过 EQ-5D-5L 量表评估)、助行器的使用、居住状况和髋关节功能(通过 Oxford 髋关节评分量表评估)产生负面影响?(3)哪些因素与初次 THA 后发生 PJI 的患者的不良患者报告结局(PROM)相关?
本研究纳入了 442 例初次 THA 后发生 PJI 的患者,这些患者来自先前发表的一项全国性研究,包括从瑞典 2005 年至 2008 年接受初次 THA 的所有患者(n=45570),这些患者均来自瑞典髋关节置换登记处(SHAR)。通过瑞典处方药物登记处识别可能的深部 PJI,并通过病历审查进行验证。对发生 PJI 的患者与未发生 PJI 的 45128 例接受初次 THA 的患者进行比较,后者的死亡率来自 SHAR,而 SHAR 的数据则每天从人口登记处更新。对 2008 年接受初次 THA 的患者进行亚组分析,以调整 ASA 评分对死亡率的影响,因为 ASA 评分在当时已在 SHAR 中可用。对于 PROM 分析,我们从每个存活的 PJI 患者中匹配了年龄、性别、手术指征和手术年份相同的三个对照组。在初次手术后平均 11 年,对 PJI 患者和对照组进行问卷调查,问卷内容包括 EQ-5D-5L 量表、助行器的使用、居住状况和 Oxford 髋关节评分量表。除年龄和性别外,我们还分析了再手术数据(如再手术次数和手术入路)和最终原位假体,以探讨可能与 PROM 结果不良相关的因素。
在控制性别、年龄和手术指征的差异后,我们发现 PJI 患者的全因 10 年死亡率(45%)高于未发生 PJI 的 THA 患者(29%)(比值比 1.4 [95% CI 1.2 至 1.6];p<0.001)。在至少 10 年的随访后,问卷调查显示 PJI 患者的 EQ-5D-5L 指数评分较低(0.83 比 0.94,-0.13 [95% CI -0.18 至 -0.08];p<0.001),辅助生活的比例较高(21% 比 12%,OR 2.0 [95% CI 1.2 至 3.3];p=0.01),需要助行器的比例较高(65% 比 42%,OR 3.1 [95% CI 2.1 至 4.8];p<0.001),Oxford 髋关节评分量表评分较低(36 比 44,-5.9 [-7.7 至 -4.0];p<0.001)。与对照组相比,PJI 患者的 Oxford 髋关节评分量表评分较低的相关因素包括:三次或以上的再手术(-8.0 [95% CI -13.0 至 -3.2];p=0.01)和初次翻修手术中使用直接外侧入路而非后侧入路(-4.3 [95% CI -7.7 至 -0.9];p=0.01)。
在这项研究中,我们发现 THA 后发生 PJI 会对死亡率、长期健康相关生活质量和髋关节功能产生负面影响。此外,亚组分析显示,可改变的因素(如再手术次数和手术入路)与髋关节功能较差相关。这强调了及时、正确的初始治疗以减少反复手术的重要性,以尽量减少髋关节 PJI 的长期负面影响。
III 级,治疗性研究。