Monash-Cabrini Department of Musculoskeletal Health and Clinical Epidemiology, School of Public Health and Preventive Medicine, Monash University, Victoria, Australia.
South Western Sydney Clinical School, University of New South Wales, Liverpool, Australia.
Clin Orthop Relat Res. 2022 Oct 1;480(10):1899-1909. doi: 10.1097/CORR.0000000000002301. Epub 2022 Jun 30.
The ability to identify which patients are at a greater risk of early revision knee arthroplasty has important practical and resource implications. Many international arthroplasty registries administer patient-reported outcome measures (PROMs) to provide a holistic assessment of pain, function, and quality of life. However, few PROM scores have been evaluated as potential indicators of early revision knee arthroplasty, and earlier studies have largely focused on knee-specific measures.
QUESTIONS/PURPOSES: This national registry-based study asked: (1) Which 6-month postoperative knee-specific and generic PROM scores are associated with early revision knee arthroplasty (defined as revision surgery performed 6 to 24 months after the primary procedure)? (2) Is a clinically important improvement in PROM scores (based on thresholds for the minimal important change) after primary knee arthroplasty associated with a lower risk of early revision?
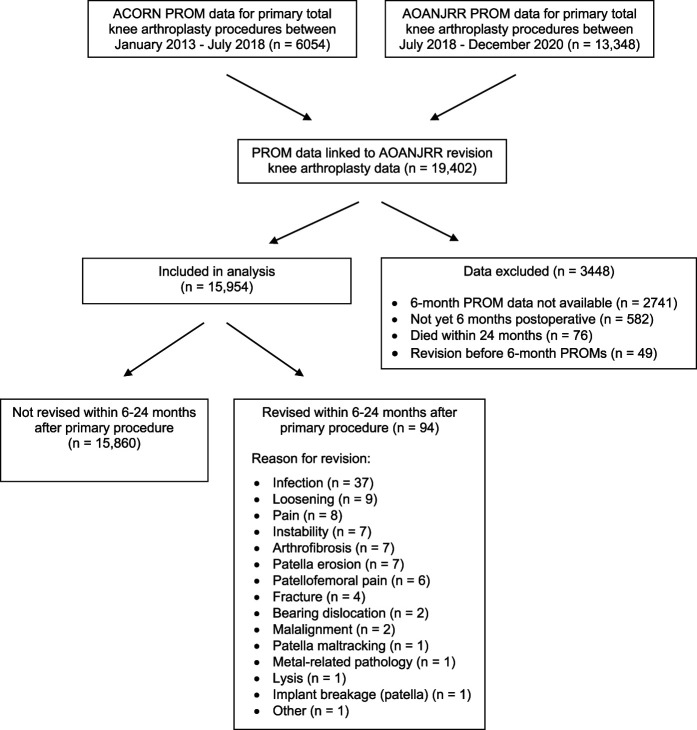
Preoperative and 6-month postoperative PROM scores for patients undergoing primary knee arthroplasty were sourced from the Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) and Arthroplasty Clinical Outcomes Registry National. Between January 2013 and December 2020, PROM data were available for 19,402 primary total knee arthroplasties; these data were linked to AOANJRR data on revision knee arthroplasty. Of these, 3448 procedures were excluded because they did not have 6-month PROM data, they had not reached the 6-month postoperative point, they had died before 24 months, or they had received revision knee arthroplasty before the 6-month PROMs assessment. After these exclusions, data were analyzed for 15,954 primary knee arthroplasties. Associations between knee-specific (knee pain, Oxford Knee Score, and 12-item Knee injury and Osteoarthritis Outcome Score [KOOS-12]) or generic PROM scores (5-level EuroQol quality of life instrument [EQ-5D], EQ VAS, perceived change, and satisfaction) and revision surgery were explored using t-tests, chi-square tests, and regression models. Ninety-four revision procedures were performed at 6 to 24 months, most commonly for infection (39% [37 procedures]). The early revision group was younger than the unrevised group (mean age 64 years versus 68 years) and a between-group difference in American Society of Anesthesiologists (ASA) grade was noted. Apart from a small difference in preoperative low back pain for the early revision group (mean low back pain VAS 4.2 points for the early revision group versus 3.3 points for the unrevised group), there were no between-group differences in preoperative knee-specific or generic PROM scores on univariate analysis. As the inclusion of ASA grade or low back pain score did not alter the model results, the final multivariable model included only the most clinically plausible confounders (age and gender) as covariates. Multivariable models (adjusting for age and gender) were also used to examine the association between a clinically important improvement in PROM scores (based on published thresholds for minimal important change) and the likelihood of early revision.
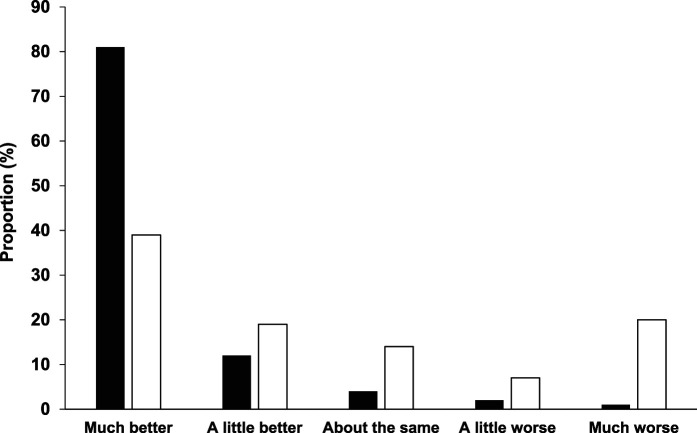
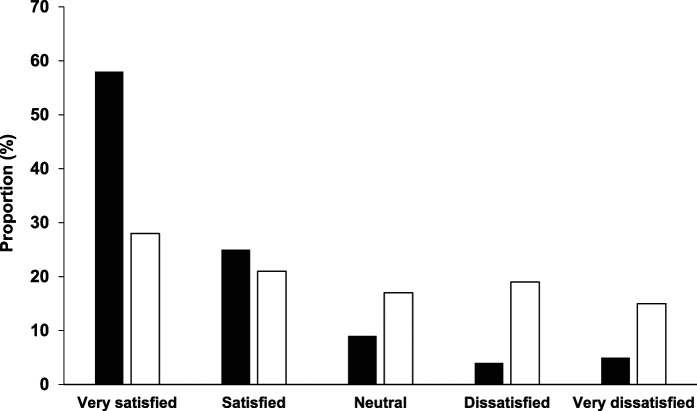
After adjusting for age and gender, poor postoperative knee pain, Oxford, KOOS-12, EQ-5D, and EQ VAS scores were all associated with early revision. A one-unit increase (worsening) in knee pain at 6 months was associated with a 31% increase in the likelihood of revision (RR 1.31 [95% confidence interval (CI) 1.19 to 1.43]; p < 0.001). Reflecting the reversed scoring direction, a one-unit increase (improvement) in Oxford or KOOS-12 score was associated with a 9% and 5% reduction in revision risk, respectively (RR for Oxford: 0.91 [95% CI 0.90 to 0.93]; p < 0.001; RR for KOOS-12 summary: 0.95 [95% CI 0.94 to 0.97]; p < 0.001). Patient dissatisfaction (RR 6.8 [95% CI 3.7 to 12.3]) and patient-perceived worsening (RR 11.7 [95% CI 7.4 to 18.5]) at 6 months were also associated with an increased likelihood of early revision. After adjusting for age and gender, patients who did not achieve a clinically important improvement in PROM scores had a higher risk of early revision (RR 2.9 for the knee pain VAS, RR 4.2 for the Oxford Knee Score, RR 6.3 to 8.6 for KOOS-12, and RR 2.3 for EQ-5D) compared with those who did (reference group).
Knee-specific and generic PROM scores offer an efficient approach to identifying patients at greater risk of early revision surgery, using either the 6-month score or the magnitude of improvement. These data indicate that surgeons can use single- and multi-item measures to detect a patient-perceived unsuccessful surgical outcome at 6 months after primary knee arthroplasty. Surgeons should be alert to poor PROM scores at 6 months or small improvements in scores (for example, less than 2 points for knee pain VAS or less than 10.5 points for Oxford Knee Score), which signal a need for direct patient follow-up or expedited clinical review.
Level III, therapeutic study.
能够识别哪些患者有更大的早期翻修膝关节置换风险具有重要的实际和资源意义。许多国际关节置换登记处都管理患者报告的结果测量(PROMs),以提供疼痛、功能和生活质量的整体评估。然而,很少有 PROM 评分被评估为早期翻修膝关节置换的潜在指标,早期研究主要集中在膝关节特异性指标上。
问题/目的:这项基于全国注册的研究提出了以下问题:(1)哪些 6 个月时的膝关节特异性和通用 PROM 评分与早期翻修膝关节置换(定义为原发性手术后 6 至 24 个月内进行的手术)相关?(2)原发性膝关节置换术后 PROM 评分是否有临床意义的改善(基于最小重要变化的阈值)是否与降低早期翻修的风险相关?
从澳大利亚矫形协会国家关节置换登记处(AOANJRR)和关节置换临床结果登记处全国获取接受原发性膝关节置换术患者的术前和 6 个月时的 PROM 数据。在 2013 年 1 月至 2020 年 12 月期间,共有 19402 例初次全膝关节置换术有 PROM 数据;这些数据与 AOANJRR 关于翻修膝关节置换的数据相关联。其中 3448 例手术因无 6 个月 PROM 数据、未达到 6 个月术后时间点、在 24 个月前死亡或在 6 个月 PROM 评估前接受了膝关节翻修手术而被排除。排除这些病例后,对 15954 例初次膝关节置换术进行了数据分析。使用 t 检验、卡方检验和回归模型,探讨了膝关节特异性(膝关节疼痛、牛津膝关节评分和 12 项膝关节损伤和骨关节炎结果评分 [KOOS-12])或通用 PROM 评分(5 级欧洲五维健康量表[EQ-5D]、EQ VAS、感知变化和满意度)与翻修手术之间的关系。94 例患者在 6 至 24 个月时进行了翻修手术,最常见的原因是感染(39%[37 例])。早期翻修组比未翻修组年轻(平均年龄 64 岁对 68 岁),并且注意到两组之间的美国麻醉医师协会(ASA)分级存在差异。除了早期翻修组术前腰痛的差异较小(平均腰痛 VAS 评分早期翻修组为 4.2 分,未翻修组为 3.3 分)外,两组间术前膝关节特异性或通用 PROM 评分在单变量分析中无差异。由于包含 ASA 分级或腰痛评分并未改变模型结果,最终多变量模型仅包括最具临床意义的混杂因素(年龄和性别)作为协变量。还使用多变量模型(调整年龄和性别)来检验 PROM 评分的临床意义改善(基于最小重要变化的已发表阈值)与早期翻修的可能性之间的关联。
在调整年龄和性别后,术后膝关节疼痛、牛津、KOOS-12、EQ-5D 和 EQ VAS 评分较差均与早期翻修相关。膝关节疼痛增加一个单位(恶化)与翻修可能性增加 31%相关(RR 1.31[95%置信区间 1.19 至 1.43];p<0.001)。反映了相反的评分方向,牛津或 KOOS-12 评分增加一个单位(改善)与翻修风险降低 9%和 5%相关(牛津 RR:0.91[95%CI 0.90 至 0.93];p<0.001;KOOS-12 综合 RR:0.95[95%CI 0.94 至 0.97];p<0.001)。患者不满(RR 6.8[95%CI 3.7 至 12.3])和患者感知恶化(RR 11.7[95%CI 7.4 至 18.5])也与早期翻修的可能性增加相关。在调整年龄和性别后,未达到 PROM 评分临床意义改善的患者发生早期翻修的风险更高(膝关节疼痛 VAS 的 RR 为 2.9,牛津膝关节评分的 RR 为 4.2,KOOS-12 的 RR 为 6.3 至 8.6,EQ-5D 的 RR 为 2.3)与达到改善的患者(参考组)相比。
膝关节特异性和通用 PROM 评分提供了一种有效的方法,可根据 6 个月时的评分或改善程度来识别更有可能接受早期翻修手术的患者。这些数据表明,外科医生可以使用单项目和多项目措施来检测原发性膝关节置换术后 6 个月时患者感知的手术结果不成功。外科医生应该警惕 6 个月时的 PROM 评分较差或评分改善较小(例如,膝关节疼痛 VAS 减少不到 2 分或牛津膝关节评分减少不到 10.5 分),这表明需要对患者进行直接随访或加快临床审查。
III 级,治疗性研究。