Lozano Rebeca, Lorente David, Aragon Isabel M, Romero-Laorden Nuria, Nombela Paz, Mateo Joaquim, Reid Alison H M, Cendón Ylenia, Bianchini Diletta, Llacer Casilda, Sandhu Shahneen K, Sharp Adam, Rescigno Pasquale, Garcés Teresa, Pacheco Maria I, Flohr Penelope, Massard Christophe, López-Casas Pedro P, Castro Elena, de Bono Johann S, Olmos David
Genitourinary Cancer Traslational Research Group, The Institute of Biomedical Research in Málaga (IBIMA), 29010 Málaga, Spain.
Spanish National Cancer Research Centre (CNIO), Prostate Cancer Clinical Research Unit, 28029 Madrid, Spain.
Cancers (Basel). 2021 May 12;13(10):2334. doi: 10.3390/cancers13102334.
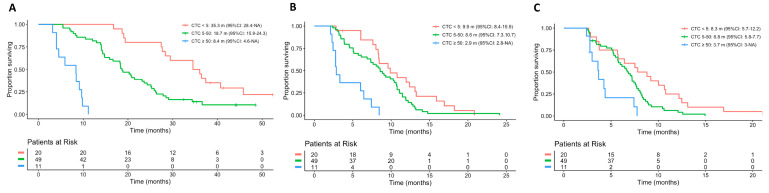
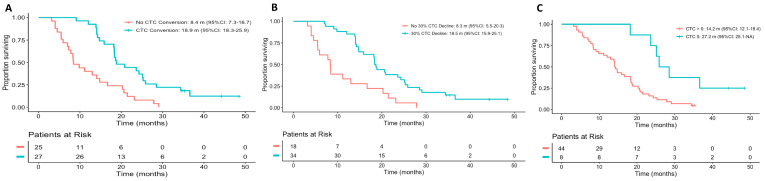
Circulating tumor cell (CTC) enumeration and changes following treatment have been demonstrated to be superior to PSA response in determining mCRPC outcome in patients receiving AR signaling inhibitors but not taxanes. We carried out a pooled analysis of two prospective studies in mCRPC patients treated with docetaxel. CTCs were measured at baseline and 3-6 weeks post treatment initiation. Cox regression models were constructed to compare 6-month radiographical progression-free survival (rPFS), CTCs and PSA changes predicting outcome. Among the subjects, 80 and 52 patients had evaluable baseline and post-treatment CTC counts, respectively. A significant association of higher baseline CTC count with worse overall survival (OS), PFS and time to PSA progression (TTPP) was observed. While CTC response at 3-6 weeks (CTC conversion (from ≥5 to <5 CTCs), CTC30 (≥30% decline in CTC) or CTC0 (decline to 0 CTC)) and 6-month rPFS were significantly associated with OS (all < 0.005), the association was not significant for PSA30 or PSA50 response. CTC and PSA response were discordant in over 50% of cases, with outcome driven by CTC response in these patients. The c-index values for OS were superior for early CTC changes compared to PSA response endpoints, and similar to 6-month rPFS. Early CTC declines were good predictors of improved outcomes in mCRPC patients treated with docetaxel in this small study, offering a superior and/or earlier estimation of docetaxel benefit in comparison to PSA or rPFS that merits further confirmation in larger studies.
循环肿瘤细胞(CTC)计数及治疗后的变化已被证明,在确定接受雄激素受体(AR)信号抑制剂而非紫杉烷类药物治疗的转移性去势抵抗性前列腺癌(mCRPC)患者的治疗结果方面,优于前列腺特异抗原(PSA)反应。我们对两项多西他赛治疗mCRPC患者的前瞻性研究进行了汇总分析。在基线期以及治疗开始后3 - 6周测量CTC。构建Cox回归模型,以比较预测6个月影像学无进展生存期(rPFS)、CTC和PSA变化的结果。在这些受试者中,分别有80例和52例患者的基线期和治疗后CTC计数可评估。观察到基线期CTC计数越高与总生存期(OS)、无进展生存期(PFS)和PSA进展时间(TTPP)越差显著相关。虽然3 - 6周时的CTC反应(CTC转换(从≥5个降至<5个CTC)、CTC30(CTC下降≥30%)或CTC0(降至0个CTC))和6个月rPFS与OS显著相关(均<0.005),但对于PSA30或PSA50反应,这种相关性并不显著。在超过50%的病例中,CTC和PSA反应不一致,这些患者的治疗结果由CTC反应驱动。与PSA反应终点相比,早期CTC变化对OS的c指数值更高,且与6个月rPFS相似。在这项小型研究中,早期CTC下降是多西他赛治疗mCRPC患者预后改善的良好预测指标,与PSA或rPFS相比,能更优和/或更早地评估多西他赛的疗效,这值得在更大规模的研究中进一步证实。