Nguyen Van Thi Khanh, Montakantikul Preecha, Tragulpiankit Pramote, Houngsaitong Jantana, Shuib Mohd Fazli
Division of Clinical Pharmacy, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok 10400, Thailand.
Pharmacy Department, FV Hospital, Hochiminh City 70000, Vietnam.
Antibiotics (Basel). 2021 May 17;10(5):595. doi: 10.3390/antibiotics10050595.
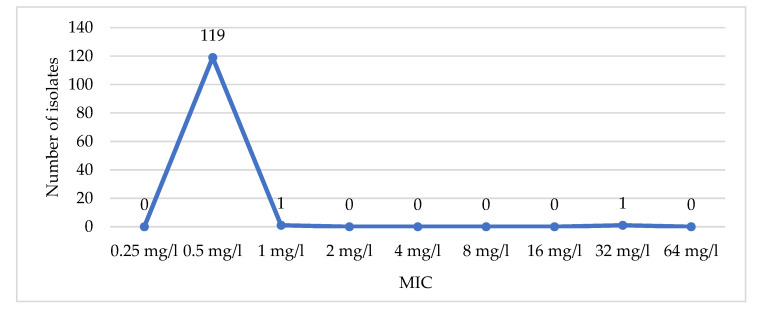
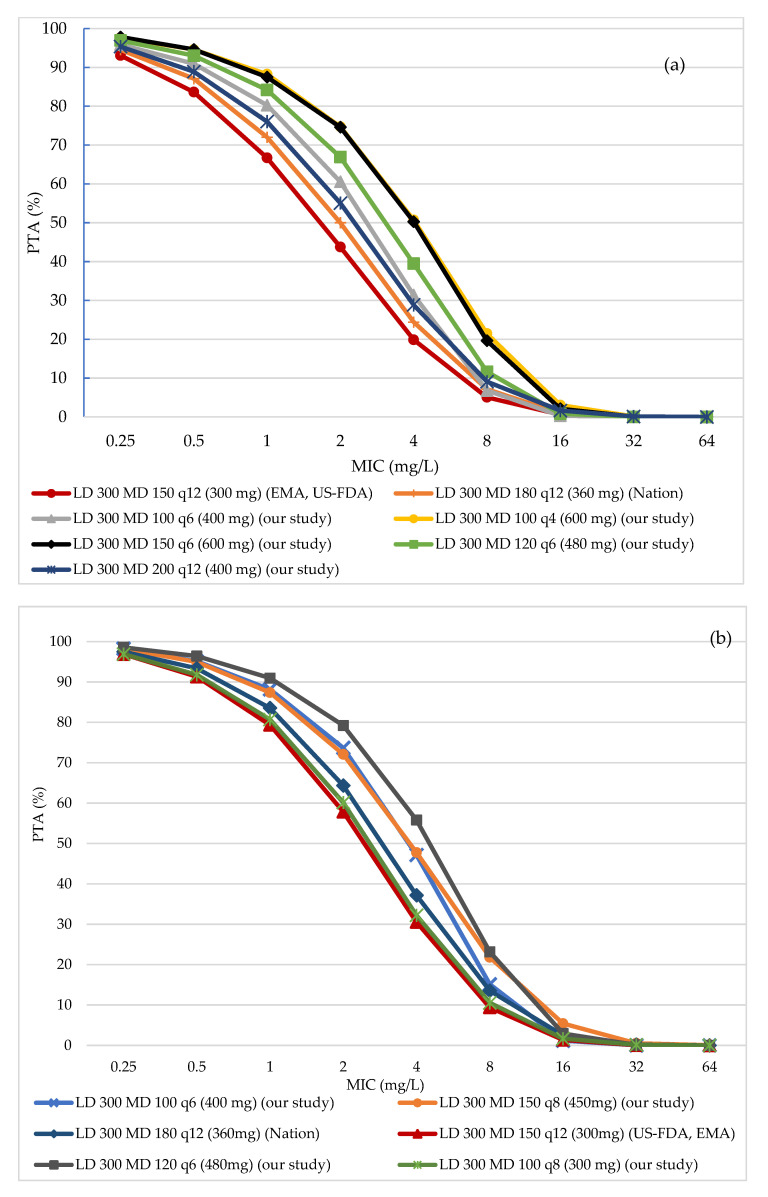
Our aims are to assess various colistin dosing regimens against () infection in critically ill patients and to propose an appropriate regimen based on microbiological data. A Monte Carlo simulation was performed using the published colistin's pharmacokinetic parameters of critically ill patients, the published pharmacodynamic target from a mouse thigh infection model, and the minimum inhibitory concentration (MIC) results from a Vietnamese hospital. The probability of target attainment (PTA) of 80% and cumulative fraction of response (CFR) of 90% were used to evaluate the efficacy of each regimen. Of 121 laboratory datasets, the carbapenem-resistant (CRPA) and the colistin-resistant rates were 29.8% and 0.8%, respectively. MIC were both 0.5 mg/L. The simulated results showed that at MIC of 2 mg/L, most regimens could not reach the PTA target, particularly in patients with normal renal function (Creatinine clearance (CrCl) ≥ 80 mL/min). At MIC of 0.5 mg/L and 1 mg/L, current recommendations still worked well. On the basis of these results, aside from lung infection, our study recommends three regimens against infection at MIC of 0.5 mg/L, 1 mg/L, and 2 mg/L. In conclusion, higher total daily doses and fractionated colistin dosing regimens could be the strategy for difficult-to-acquire PTA cases, while a less aggressive dose might be appropriate for empirical treatment in settings with low MIC.
我们的目标是评估针对重症患者()感染的各种黏菌素给药方案,并根据微生物学数据提出合适的方案。使用已发表的重症患者黏菌素药代动力学参数、小鼠大腿感染模型中已发表的药效学靶点以及越南一家医院的最低抑菌浓度(MIC)结果进行了蒙特卡洛模拟。采用80%的达标概率(PTA)和90%的累积反应分数(CFR)来评估每种方案的疗效。在121个实验室数据集中,耐碳青霉烯类(CRPA)和耐黏菌素的比例分别为29.8%和0.8%。MIC均为0.5 mg/L。模拟结果表明,在MIC为2 mg/L时,大多数方案无法达到PTA目标,尤其是在肾功能正常(肌酐清除率(CrCl)≥80 mL/min)的患者中。在MIC为0.5 mg/L和1 mg/L时,目前的推荐方案仍然有效。基于这些结果,除肺部感染外,我们的研究推荐了针对MIC为0.5 mg/L、1 mg/L和2 mg/L的()感染的三种方案。总之,较高的每日总剂量和黏菌素分次给药方案可能是难以达到PTA情况的策略,而在MIC较低的情况下,较温和的剂量可能适合经验性治疗。