Sica Antonello, Casale Beniamino, Sagnelli Caterina, Di Dato Maria Teresa, Rispoli Marco, Santagata Mario, Buonavolontà Pietro, Fiorelli Alfonso, Vitiello Paola, Caccavale Stefano, Creta Massimiliano, Salzano Anna Maria, Sagnelli Evangelista, Saracco Elisabetta, Gazzerro Giuseppe, Famiglietti Vincenzo, Tammaro Dario, Papa Alfonso
Department of Precision Medicine, University of Campania Luigi Vanvitelli, 80131 Naples, Italy.
Department of Pneumology and Tisiology, AORN Dei Colli-V. Monaldi, 80131 Naples, Italy.
Healthcare (Basel). 2021 May 18;9(5):589. doi: 10.3390/healthcare9050589.
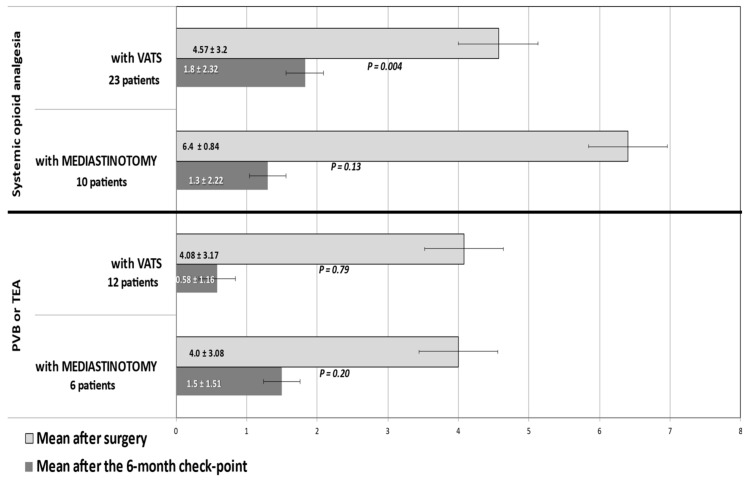
Chest pain following a trans-thoracic biopsy often has multiple etiologies, especially in patients with lymphomas. Pathological neuronal mechanisms integrate with an overproduction of IL-6, TNF-α, IL1-β by macrophages and monocytes, which amplifies inflammation and pain. In consideration of this complex pathogenesis, international guidelines recommend diversified analgesia protocols: thoracic epidural, paravertebral block, and systemic administration of opioids. This study reports an attempt to reduce chest pain and prevent chronic pain in 51 patients undergoing trans-thoracic biopsy for mediastinal lymphoma. The entity of pain, measured 72nd hour after biopsy by the Numerical Rating Scale (NRS), was compared with that seen at a 6th month checkpoint in 46 patients. The pain decreased in all cases. At the 6th month checkpoint, among 31 opioid-treated patients, none of the 16 patients with NRS < 6 within the 72nd hour post biopsy had developed chronic chest pain, while 8 of the 15 with higher values did ( < 0.01). Of 10 patients undergoing thoracotomy and treated with opioids, eight had a NRS of no more than 2, of which six had no chronic pain. Of the twenty-one patients who underwent VATS biopsy and were treated with opioids, fifteen had NRS no greater than 2, of which ten had no chronic pain. Subgroups of patients biopsied under mediastinotomy or video-assisted thoracoscopic surgery (VATS) and treated with thoracic epidural analgesia (TEA) or PVB were too small for such analysis.
经胸活检后的胸痛通常有多种病因,在淋巴瘤患者中尤为如此。病理神经元机制与巨噬细胞和单核细胞过度产生白细胞介素-6(IL-6)、肿瘤坏死因子-α(TNF-α)、白细胞介素-1β(IL1-β)相互作用,从而加剧炎症和疼痛。鉴于这种复杂的发病机制,国际指南推荐采用多样化的镇痛方案:胸段硬膜外阻滞、椎旁阻滞和全身性使用阿片类药物。本研究报告了一项针对51例因纵隔淋巴瘤接受经胸活检患者减轻胸痛并预防慢性疼痛的尝试。通过数字评分量表(NRS)在活检后第72小时测量的疼痛程度,与46例患者在第6个月检查点时的疼痛程度进行了比较。所有病例的疼痛均有所减轻。在第6个月检查点时,在31例接受阿片类药物治疗的患者中,活检后第72小时内NRS<6的16例患者均未出现慢性胸痛,而NRS较高的15例患者中有8例出现了慢性胸痛(P<0.01)。在10例接受开胸手术并接受阿片类药物治疗的患者中,8例NRS不超过2,其中6例没有慢性疼痛。在21例接受电视辅助胸腔镜手术(VATS)活检并接受阿片类药物治疗的患者中,15例NRS不超过2,其中10例没有慢性疼痛。在纵隔切开术或电视辅助胸腔镜手术(VATS)下进行活检并接受胸段硬膜外镇痛(TEA)或椎旁阻滞(PVB)治疗的患者亚组太小,无法进行此类分析。