Ornello Raffaele, De Matteis Eleonora, Di Felice Chiara, Caponnetto Valeria, Pistoia Francesca, Sacco Simona
Neuroscience Section, Department of Applied Clinical Sciences and Biotechnology, University of L'Aquila, 67100 L'Aquila, Italy.
J Clin Med. 2021 May 24;10(11):2263. doi: 10.3390/jcm10112263.
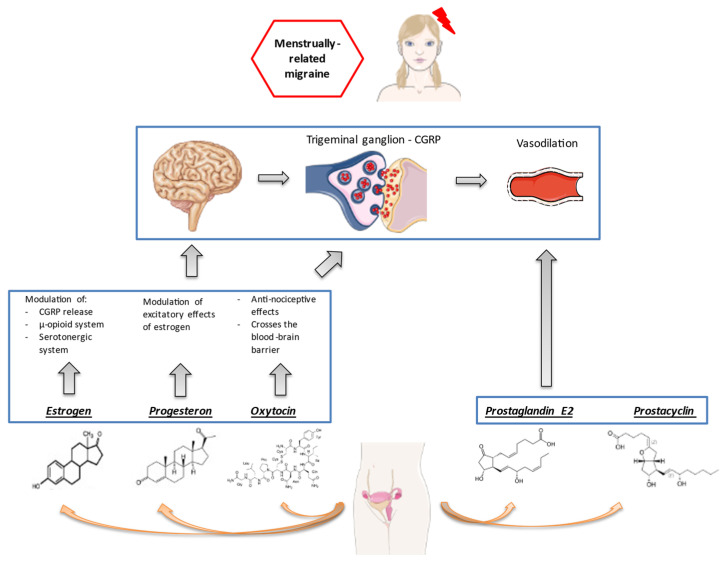
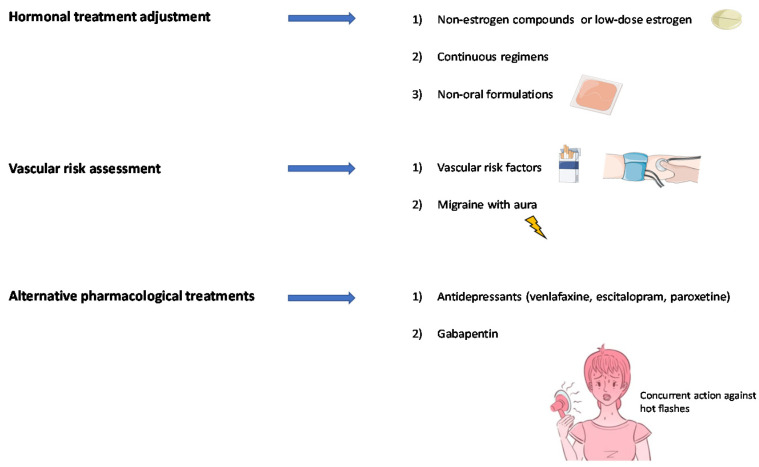
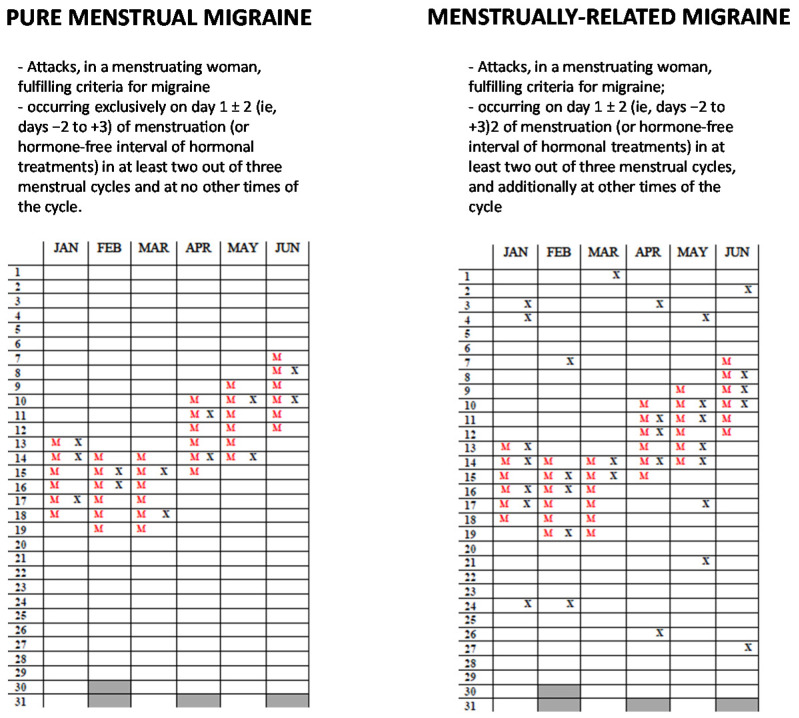
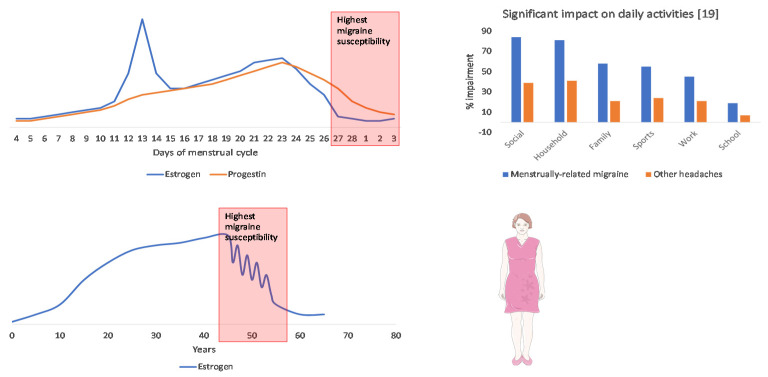
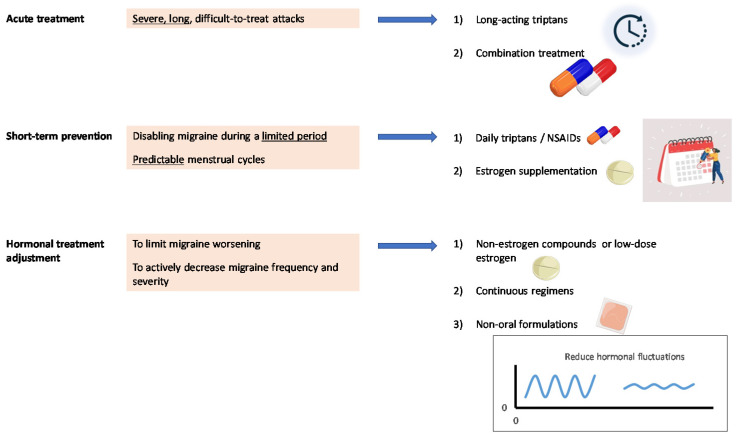
Migraine course is influenced by female reproductive milestones, including menstruation and perimenopause; menstrual migraine (MM) represents a distinct clinical entity. Increased susceptibility to migraine during menstruation and in perimenopause is probably due to fluctuations in estrogen levels. The present review provides suggestions for the treatment of MM and perimenopausal migraine. MM is characterized by long, severe, and poorly treatable headaches, for which the use of long-acting triptans and/or combined treatment with triptans and common analgesics is advisable. Short-term prophylaxis with triptans and/or estrogen treatment is another viable option in women with regular menstrual cycles or treated with combined hormonal contraceptives; conventional prevention may also be considered depending on the attack-related disability and the presence of attacks unrelated to menstruation. In women with perimenopausal migraine, hormonal treatments should aim at avoiding estrogen fluctuations. Future research on migraine treatments will benefit from the ascertainment of the interplay between female sex hormones and the mechanisms of migraine pathogenesis, including the calcitonin gene-related peptide pathway.
偏头痛病程受女性生殖阶段的影响,包括月经和围绝经期;月经性偏头痛(MM)是一种独特的临床实体。月经期间和围绝经期偏头痛易感性增加可能是由于雌激素水平波动所致。本综述为MM和围绝经期偏头痛的治疗提供了建议。MM的特点是头痛持续时间长、程度严重且难以治疗,对此建议使用长效曲坦类药物和/或曲坦类药物与普通镇痛药联合治疗。对于月经周期规律或采用复方激素避孕药治疗的女性,曲坦类药物短期预防性治疗和/或雌激素治疗是另一种可行选择;也可根据发作相关的功能障碍以及是否存在与月经无关的发作情况考虑采用传统预防方法。对于围绝经期偏头痛女性,激素治疗应旨在避免雌激素波动。未来关于偏头痛治疗的研究将受益于确定女性性激素与偏头痛发病机制之间的相互作用,包括降钙素基因相关肽途径。