Cardiovascular Institute, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, USA.
J Clin Hypertens (Greenwich). 2021 Jul;23(7):1335-1343. doi: 10.1111/jch.14296. Epub 2021 Jun 2.
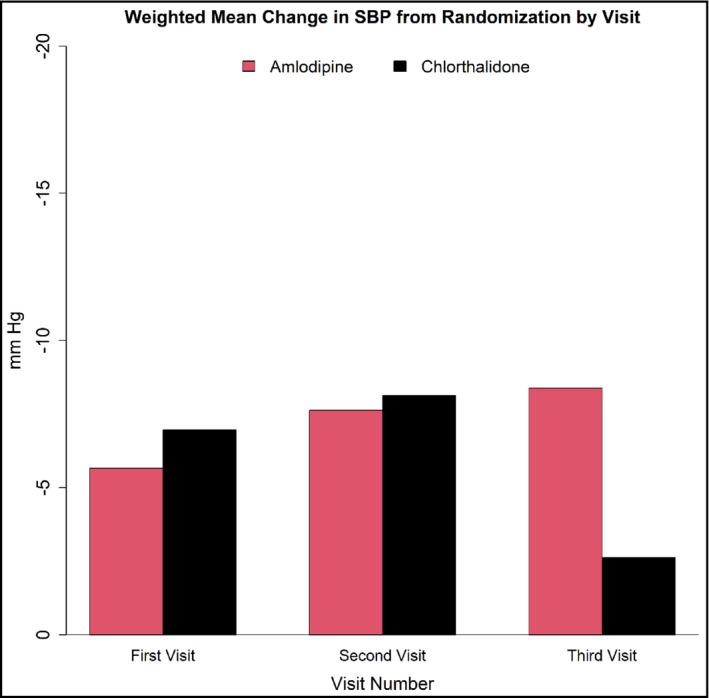
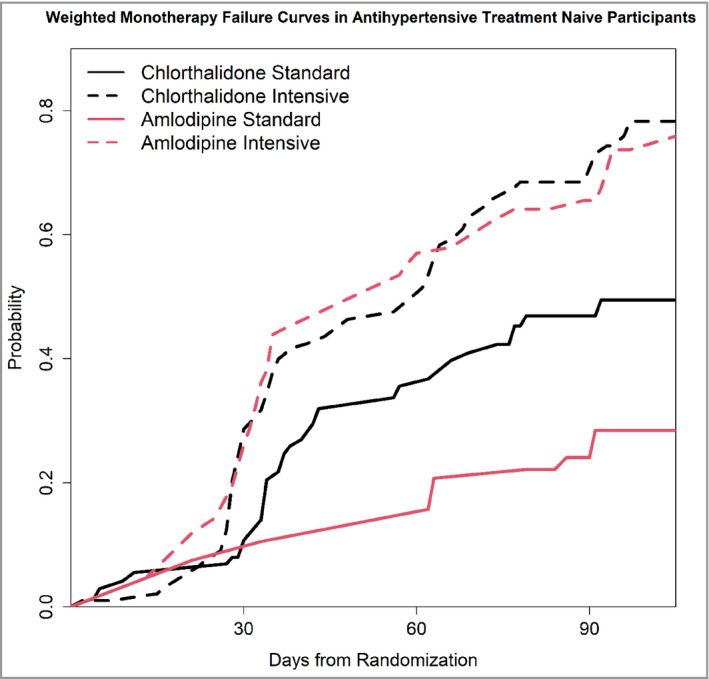
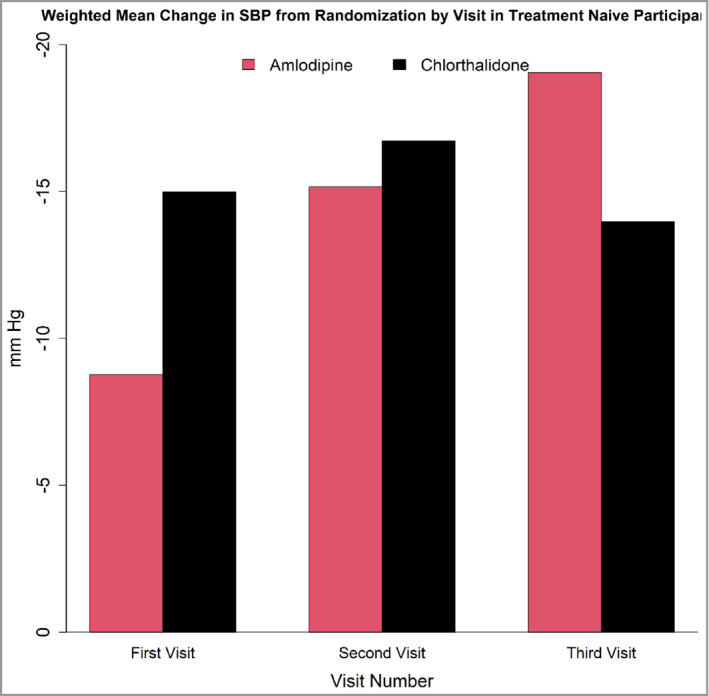
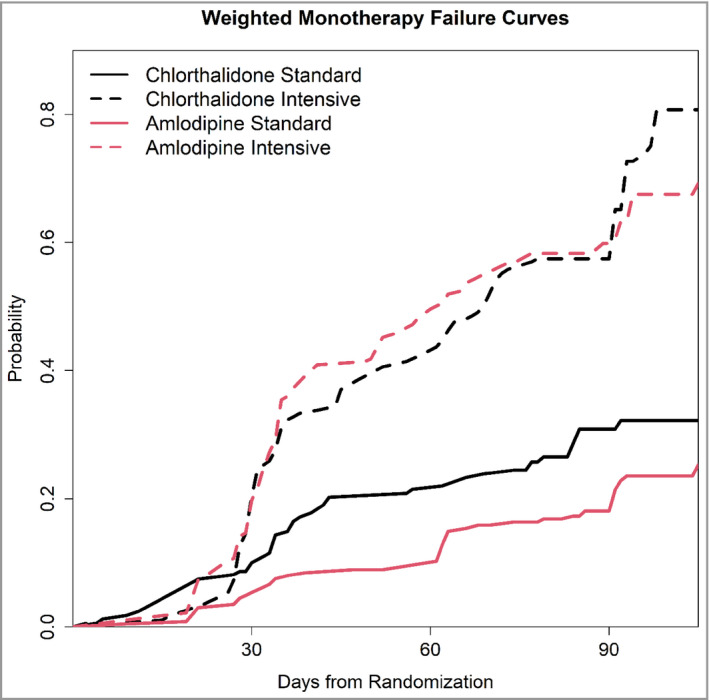
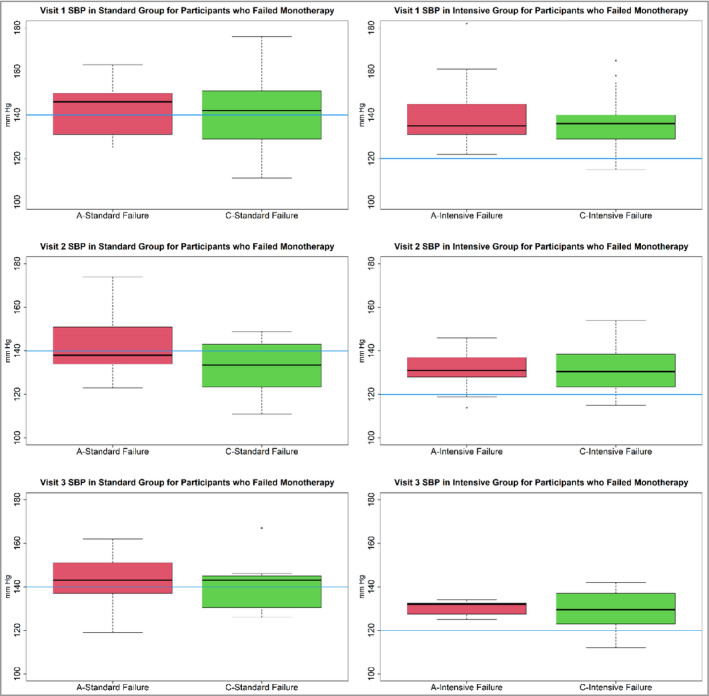
This post hoc analysis of the Systolic Blood Pressure Intervention Trial (SPRINT) examined the performance of chlorthalidone (C) versus amlodipine (A) monotherapies. ANOVA was used to analyze the differences in systolic blood pressure (SBP) response between C and A. Logistic regression was used to examine monotherapy failure (adding a second antihypertensive agent or switching to a different antihypertensive agent) rates. Four hundred ninety-one participants were treated with C monotherapy (n = 210, mean dose = 22 mg/day) or A monotherapy (n = 281, mean dose = 7 mg/day). There was a significant difference in mean SBP reduction between the C and A monotherapies at the third visit (higher reduction with A, adjusted p = .018). Unadjusted analysis showed a higher failure with C in the standard treatment group. Although the average SBP at failure was higher and above the 140 mm Hg cutoff that indicated monotherapy failure with A (142.60) compared with C (138.40), more participants on C failed despite having SBP below the 140 cutoff. This was probably due to decisions made by the investigative teams to change the antihypertensive regimen, because, in their opinion, the clinical picture required it. After adjusting for baseline characteristics, C had higher failure than A only in the standard treatment group (1.64 odds ratio [OR], 95% CI 1.06-2.56, p = .028). A sub-analysis including participants who had never used antihypertensive treatment before randomization had similar results (2.57 OR, 95% CI 1.34-5.02, p = .004). Overall, in SPRINT chlorthalidone was associated with higher monotherapy failure than amlodipine in the standard treatment group because of decisions of the investigative teams.
这篇 SPRINT 事后分析检查了氯噻酮(C)与氨氯地平(A)单药治疗的效果。方差分析用于分析 C 和 A 单药治疗组收缩压(SBP)反应的差异。逻辑回归用于检查单药治疗失败(加用第二种降压药或改用其他降压药)率。491 名患者接受氯噻酮单药治疗(n=210,平均剂量 22mg/天)或氨氯地平单药治疗(n=281,平均剂量 7mg/天)。在第三次就诊时,C 和 A 单药治疗的平均 SBP 降低有显著差异(A 降低更多,调整后 p=0.018)。未经调整的分析显示标准治疗组 C 的失败率更高。尽管 C 的平均失败 SBP 更高,高于 A 单药治疗失败的 140mmHg 切点(142.60mmHg),但更多 C 组患者尽管 SBP 低于 140mmHg 切点仍失败。这可能是由于研究团队决定改变降压方案,因为根据他们的临床判断需要改变。在调整基线特征后,只有在标准治疗组中 C 的失败率才高于 A(1.64 比值比[OR],95%CI 1.06-2.56,p=0.028)。一项包括随机分组前从未使用过降压治疗的参与者的亚分析得出了相似的结果(2.57 OR,95%CI 1.34-5.02,p=0.004)。总的来说,在 SPRINT 研究中,由于研究团队的决策,氯噻酮在标准治疗组中与更高的单药治疗失败率相关。