Department of Neurology and Neurosurgery, Brain Center, University Medical Center Utrecht, the Netherlands (S.M.U.V., H.B.v.d.W.).
Department of Radiology, Maastricht University Medical Center Plus, the Netherlands (A.A.P.).
Stroke. 2021 Aug;52(9):2849-2857. doi: 10.1161/STROKEAHA.120.033334. Epub 2021 Jun 3.
Cerebral white matter lesions (WMLs) have been associated with a greater risk of poor functional outcome after ischemic stroke. We assessed the relations between WML burden and radiological and clinical outcomes in patients treated with endovascular treatment in routine practice.
We analyzed data from the MR CLEAN Registry (Multicenter Randomized Controlled Trial of Endovascular Treatment for Acute Ischaemic Stroke in the Netherlands)—a prospective, multicenter, observational cohort study of patients treated with endovascular treatment in the Netherlands. WMLs were graded on baseline noncontrast computed tomography using a visual grading scale. The primary outcome was the score on the modified Rankin Scale at 90 days. Secondary outcomes included early neurological recovery, successful reperfusion (extended Thrombolysis in Cerebral Infarction ≥2b), futile recanalization (modified Rankin Scale score ≥3 despite successful reperfusion), and occurrence of symptomatic intracranial hemorrhage. We used multivariable logistic regression models to assess associations between WML severity and outcomes, taking the absence of WML on noncontrast computed tomography as the reference category.
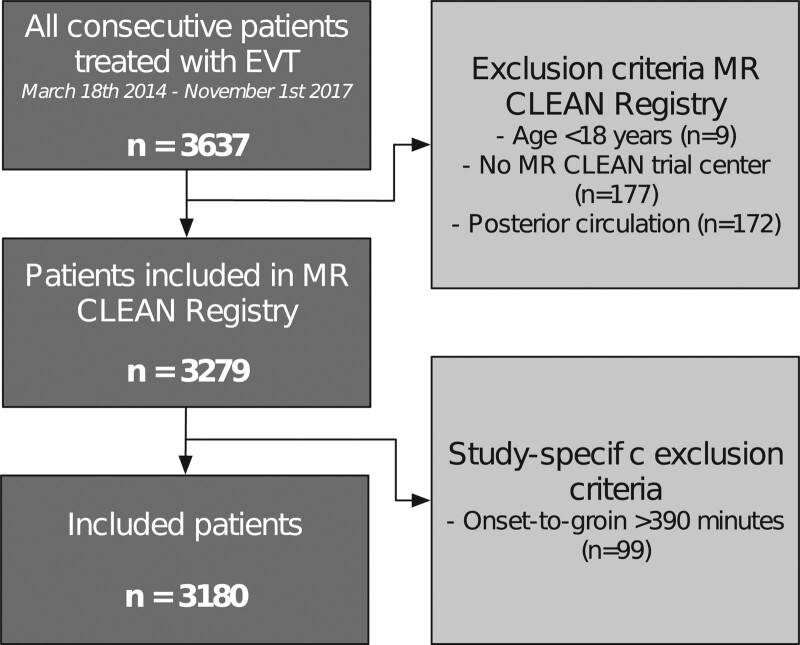
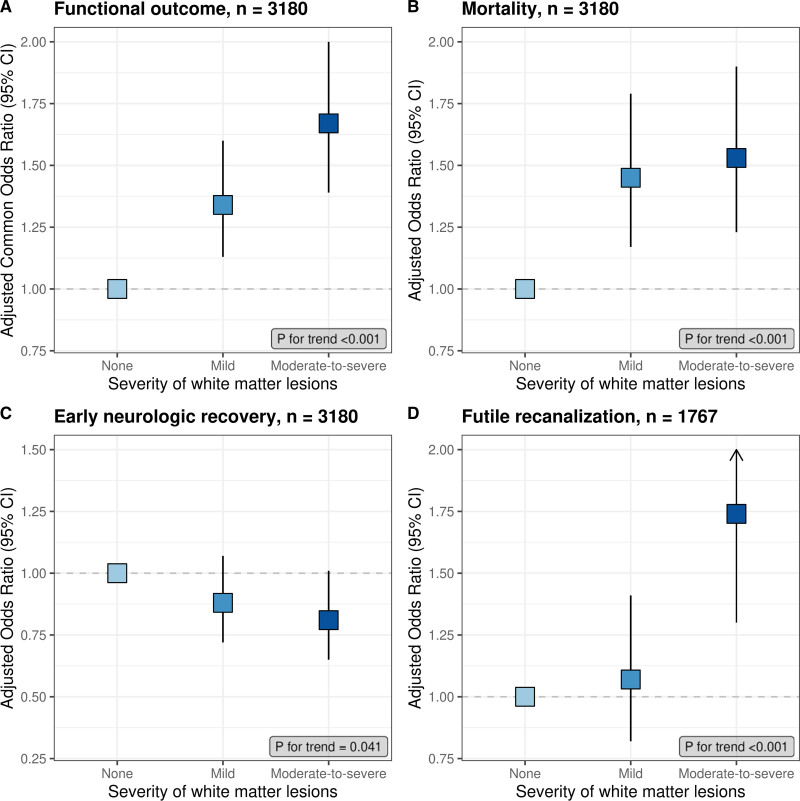
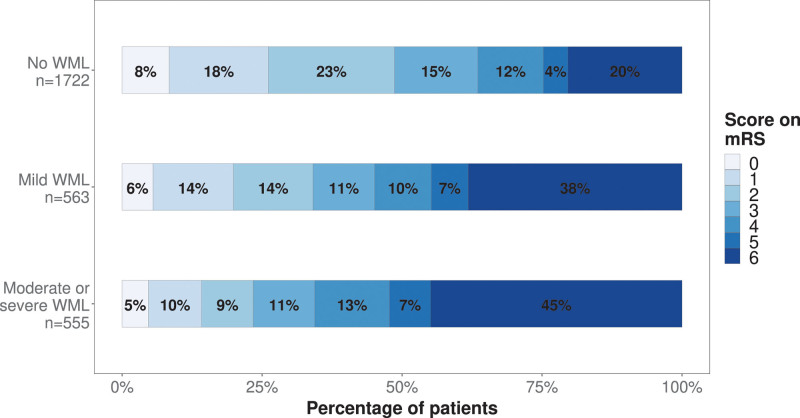
Of 3180 patients included in the MR CLEAN Registry between March 2014 and November 2017, WMLs were graded for 3046 patients and categorized as none (n=1855; 61%), mild (n=608; 20%), or moderate to severe (n=588; 19%). Favorable outcome (modified Rankin Scale score, 0–2) was achieved in 838 patients (49%) without WML, 192 patients (34%) with mild WML, and 130 patients (24%) with moderate-to-severe WML. Increasing WML grades were associated with a shift toward poorer functional outcome in a dose-dependent manner (adjusted common odds ratio, 1.34 [95% CI, 1.13–1.60] for mild WML and 1.67 [95% CI, 1.39–2.01] for moderate-to-severe WML; Ptrend, <0.001). Increasing WML grades were associated with futile recanalization (Ptrend, <0.001) and were inversely associated with early neurological recovery (Ptrend, 0.041) but not with the probability of successful reperfusion or symptomatic intracranial hemorrhage.
An increasing burden of WML at baseline is associated with poorer clinical outcomes after endovascular treatment for acute ischemic stroke but not with the probability of successful reperfusion or symptomatic intracranial hemorrhage.
脑白质病变(WML)与缺血性卒中后功能预后不良的风险增加有关。我们评估了在常规实践中接受血管内治疗的患者的 WML 负担与影像学和临床结局之间的关系。
我们分析了来自 MR CLEAN 登记研究(荷兰多中心随机对照急性缺血性卒中血管内治疗试验)的数据 - 这是一项在荷兰接受血管内治疗的患者的前瞻性、多中心、观察性队列研究。使用视觉评分量表在基线非对比 CT 上对 WML 进行分级。主要结局是 90 天时改良 Rankin 量表评分。次要结局包括早期神经恢复、成功再灌注(扩展血栓溶解治疗脑梗死 ≥2b)、无效再通(尽管成功再灌注但改良 Rankin 量表评分≥3)和症状性颅内出血的发生。我们使用多变量逻辑回归模型来评估 WML 严重程度与结局之间的关系,将非对比 CT 上无 WML 作为参考类别。
在 2014 年 3 月至 2017 年 11 月期间纳入的 3180 例患者中,对 3046 例患者进行了 WML 分级,并将其分为无 WML(n=1855;61%)、轻度(n=608;20%)或中重度(n=588;19%)。无 WML 的 838 例患者(49%)、轻度 WML 的 192 例患者(34%)和中重度 WML 的 130 例患者(24%)实现了良好结局(改良 Rankin 量表评分 0-2)。WML 分级呈剂量依赖性与较差的功能结局相关(轻度 WML 的调整后常见比值比,1.34[95%CI,1.13-1.60];中重度 WML 的调整后常见比值比,1.67[95%CI,1.39-2.01];Ptrend,<0.001)。WML 分级增加与无效再通相关(Ptrend,<0.001),与早期神经恢复呈负相关(Ptrend,0.041),但与成功再灌注的概率或症状性颅内出血无关。
基线时 WML 负担的增加与急性缺血性卒中血管内治疗后的临床结局较差相关,但与成功再灌注的概率或症状性颅内出血无关。