Ta-Tang Thuy-Huong, Luz Sergio L B, Crainey James L, Rubio José M
Malaria and NTDs Laboratory, National Centre of Tropical Medicine, Instituto de Salud Carlos III, Madrid, Spain.
Laboratório de Ecologia de Doenças Transmissíveis na Amazônia, Instituto Leônidas e Maria Deane, Fundação Oswaldo Cruz, Manaus, Amazonas State, Brazil.
Res Rep Trop Med. 2021 May 24;12:93-105. doi: 10.2147/RRTM.S274684. eCollection 2021.
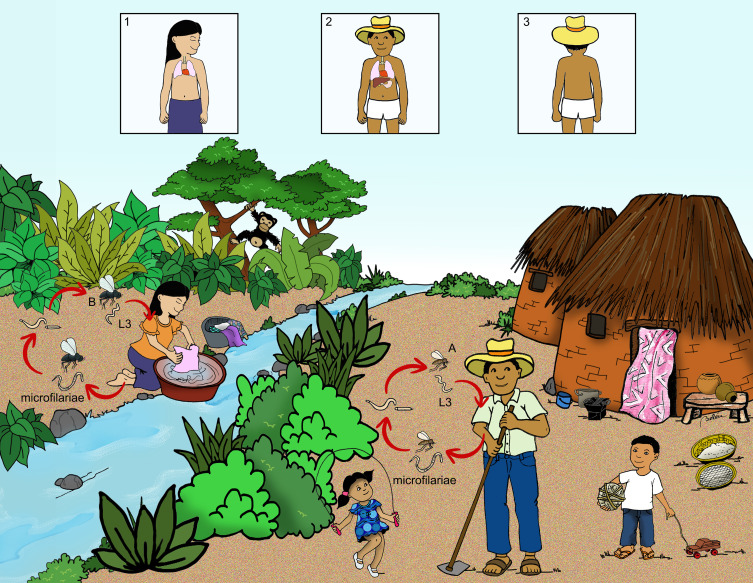
Mansonellosis is caused by three filarial parasite species from the genus that commonly produce chronic human microfilaraemias: and . The disease is widespread in Africa, the Caribbean and South and Central America, and although it is typically asymptomatic it has been associated with mild pathologies including leg-chills, joint-pains, headaches, fevers, and corneal lesions. No robust mansonellosis disease burden estimates have yet been made and the impact the disease has on blood bank stocks and the monitoring of other filarial diseases is not thought to be of sufficient public health importance to justify dedicated disease management interventions. Mansonellosis´s Ceratopogonidae and Simuliidae vectors are not targeted by other control programmes and because of their small size and out-door biting habits are unlikely to be affected by interventions targeting other disease vectors like mosquitoes. The ivermectin and mebendazole-based mass drug administration (iMDA and mMDA) treatment regimens deployed by the WHO´s Elimination of Neglected Tropical Diseases (ESPEN) programme and its forerunners have, however, likely impacted significantly on the mansonellosis disease burden, principally by reducing the transmission of in Africa. The increasingly popular plan of using iMDA to control malaria could also affect parasite prevalence and transmission in Latin America in the future. However, a potentially far greater mansonellosis disease burden impact is likely to come from short-course curative anti- therapeutics, which are presently being developed for onchocerciasis and lymphatic filariasis treatment. Even if the WHO´s ESPEN programme does not choose to deploy these drugs in MDA interventions, they have the potential to dramatically increase the financial and logistical feasibility of effective mansonellosis management. There is, thus, now a fresh and urgent need to better characterise the disease burden and eco-epidemiology of mansonellosis so that effective management programmes can be designed, advocated for and implemented.
曼氏丝虫病由曼氏属的三种丝虫寄生虫引起,这些寄生虫通常会导致人类慢性微丝蚴血症:奥氏曼森线虫、链尾曼森线虫和常现曼森线虫。该病在非洲、加勒比地区以及南美洲和中美洲广泛传播,虽然通常无症状,但它与一些轻微病症有关,包括腿部发冷、关节疼痛、头痛、发烧和角膜病变。目前尚未对曼氏丝虫病的疾病负担进行可靠估计,并且认为该疾病对血库储备以及其他丝虫病监测的影响在公共卫生方面的重要性不足以证明需要专门的疾病管理干预措施。曼氏丝虫病的蠓科和蚋科传播媒介未被其他控制项目列为目标,并且由于它们体型小和户外叮咬习性,不太可能受到针对蚊子等其他疾病传播媒介的干预措施的影响。然而,世界卫生组织消除被忽视热带病(ESPEN)项目及其前身所采用的基于伊维菌素和甲苯达唑的大规模药物给药(iMDA和mMDA)治疗方案,可能对曼氏丝虫病的疾病负担产生了重大影响,主要是通过减少非洲的常现曼森线虫传播。未来,越来越流行的使用iMDA控制疟疾的计划也可能影响拉丁美洲的寄生虫流行率和传播。然而,可能对曼氏丝虫病疾病负担产生更大影响的可能来自短期治愈性抗丝虫治疗药物,目前正在开发这些药物用于治疗盘尾丝虫病和淋巴丝虫病。即使世界卫生组织的ESPEN项目不选择在MDA干预措施中使用这些药物,它们也有可能显著提高有效管理曼氏丝虫病的财务和后勤可行性。因此,现在迫切需要更好地描述曼氏丝虫病的疾病负担和生态流行病学,以便能够设计、倡导和实施有效的管理方案。