Alexandre André R, Rocha Filipa R, Landeiro Luís, Mota Pedro, Jones Joana, Gomes José A
All authors: Department of Intensive Care, Hospital da Luz - Lisboa, Lisboa, Portugal.
Crit Care Explor. 2021 May 12;3(5):e0422. doi: 10.1097/CCE.0000000000000422. eCollection 2021 May.
The current standard of care to deliver invasive mechanical ventilation support is the protective ventilation approach. One pillar of this approach is the limitation of tidal volume to less than 6 mL/Kg of predicted body weight. Predicted body weight is calculated from patient's height. Yet, little is known about the potential impact of errors arising from visual height estimation, a common practice, to calculate tidal volumes. The aim of this study was to evaluate that impact on tidal volume calculation to use during protective ventilation.
Prospective observational study.
An eight-bed polyvalent ICU.
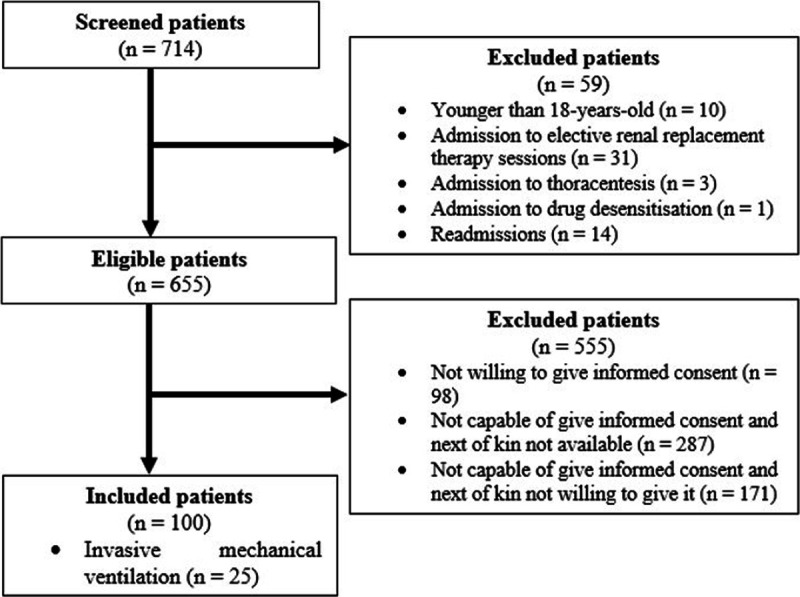
Adult patients (≥ 18 yr).
None.
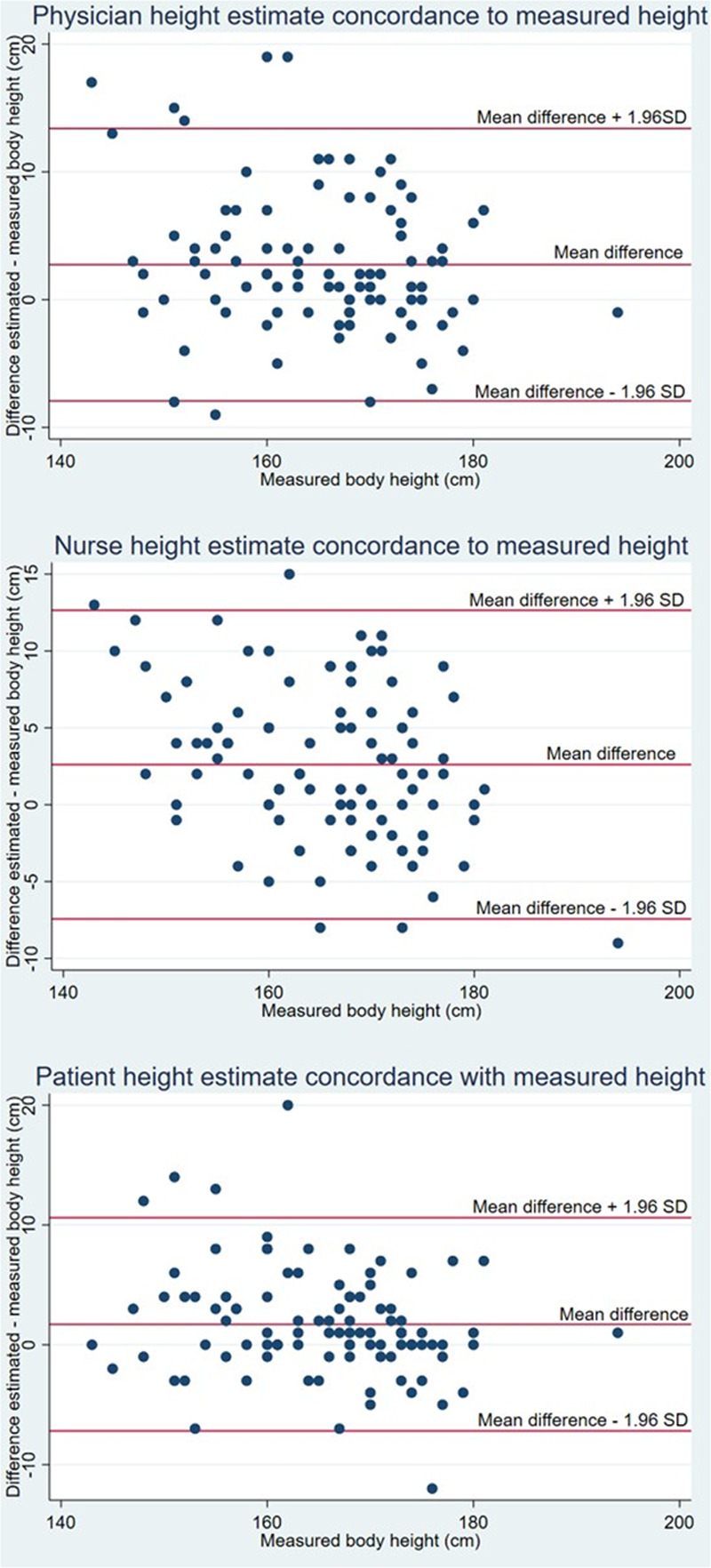
Tidal volumes were calculated from visual height estimates made by physicians, nurses, and patients themselves and compared with tidal volumes calculated from measured heights. Comparisons were made using the paired t test. Modified Bland-Altman plots were used to assess agreement between height estimates and measurements. One-hundred patients were recruited. Regardless of the height estimator, all the mean tidal volumes would be greater than 6 mL/Kg predicted body weight (all < 0.001). Additionally, tidal volumes would be greater than or equal to 6.5 mL/Kg predicted body weight in 18% of patients' estimates, 25% of physicians' estimates, and 30% of nurses' estimates. Patients with lower stature (< 165 cm), older age, and surgical typology of admission were at increased risk of being ventilated with tidal volumes above protective threshold.
The clinical benefit of the protective ventilation strategy can be offset by using visual height estimates to calculate tidal volumes. Additionally, this approach can be harmful and potentially increase mortality by exposing patients to tidal volumes greater than or equal to 6.5 mL/Kg predicted body weight. In the interest of patient safety, every ICU patient should have his or her height accurately measured.
提供有创机械通气支持的当前护理标准是保护性通气方法。该方法的一个支柱是将潮气量限制在低于预测体重的6 mL/kg。预测体重是根据患者身高计算得出的。然而,对于通过视觉估计身高(一种常用做法)来计算潮气量所产生的误差的潜在影响,人们知之甚少。本研究的目的是评估这种影响对保护性通气期间潮气量计算的作用。
前瞻性观察性研究。
一个拥有八张床位的多科室重症监护病房。
成年患者(≥18岁)。
无。
根据医生、护士和患者自己进行的视觉身高估计计算潮气量,并与根据测量身高计算的潮气量进行比较。使用配对t检验进行比较。改良的布兰德-奥特曼图用于评估身高估计值与测量值之间的一致性。招募了100名患者。无论身高估计者是谁,所有平均潮气量均会大于预测体重的6 mL/kg(均P<0.001)。此外,在患者估计值的18%、医生估计值的25%和护士估计值的30%中,潮气量会大于或等于预测体重的6.5 mL/kg。身材较矮(<165 cm)、年龄较大以及入院手术类型的患者接受高于保护阈值潮气量通气的风险增加。
使用视觉身高估计来计算潮气量可能会抵消保护性通气策略的临床益处。此外,这种方法可能有害,并可能通过使患者暴露于大于或等于预测体重的6.5 mL/kg的潮气量中而增加死亡率。为了患者安全,每个重症监护病房患者都应准确测量其身高。