Department of Ophthalmology, Universitair Ziekenhuis Brussel, Vrije Universiteit Brussel, Laarbeeklaan 101, 1090, Jette, Belgium.
Department of Medical Oncology, Universitair Ziekenhuis Brussel, Vrije Universiteit Brussel, Jette, Belgium.
BMC Ophthalmol. 2021 Jun 5;21(1):250. doi: 10.1186/s12886-021-02011-4.
The use of immunomodulating therapy to treat various cancers has been on the rise and these immune checkpoint inhibitors are known to cause ocular side effects. In this article a case of acute exudative polymorphous vitelliform maculopathy (AEPVM) is reported which developed during a first line treatment with pembrolizumab.
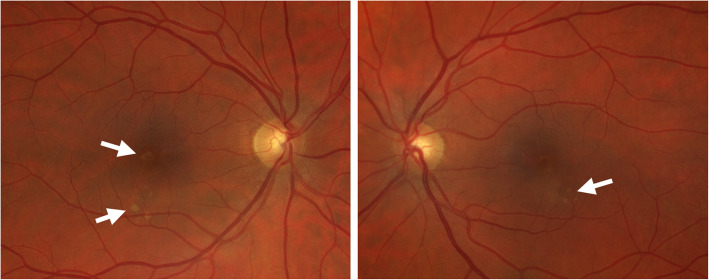
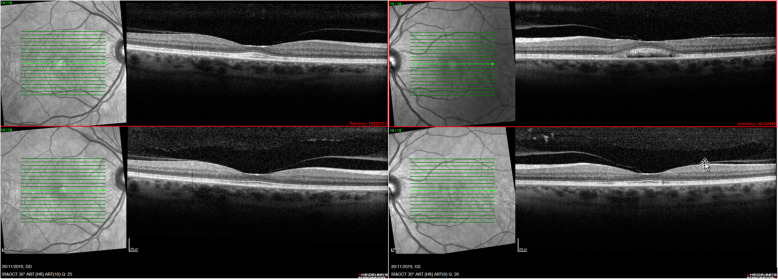
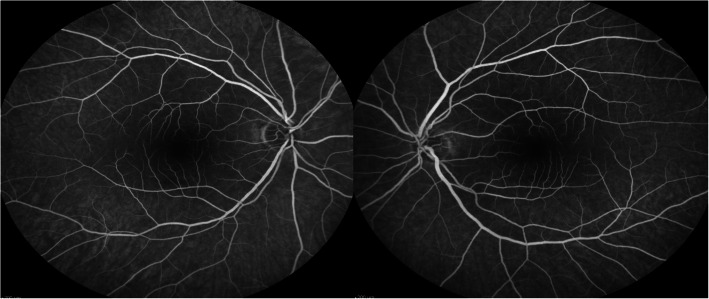
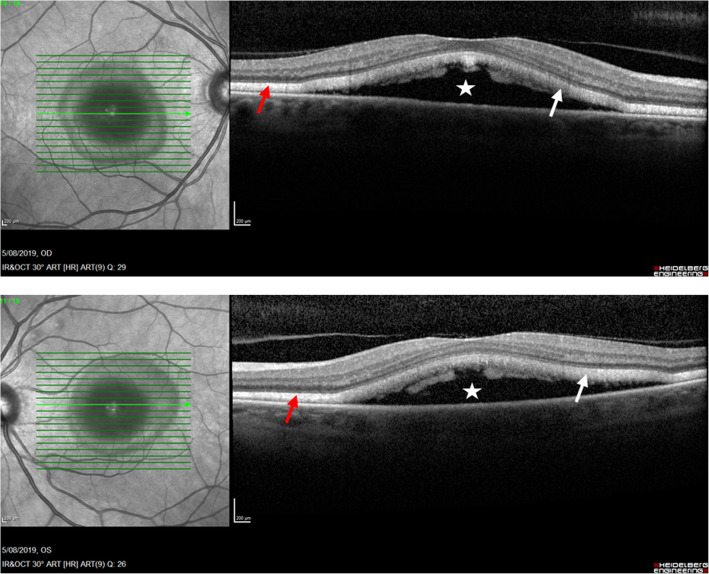
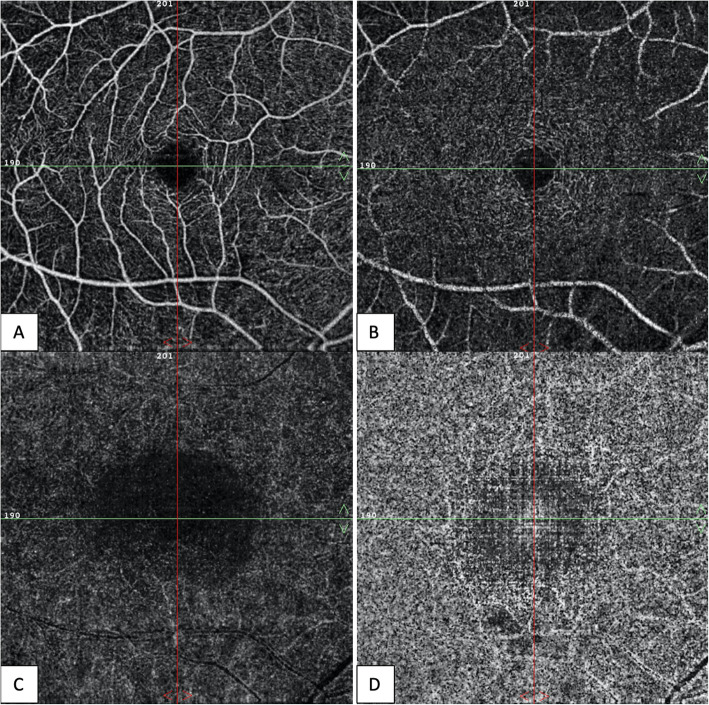
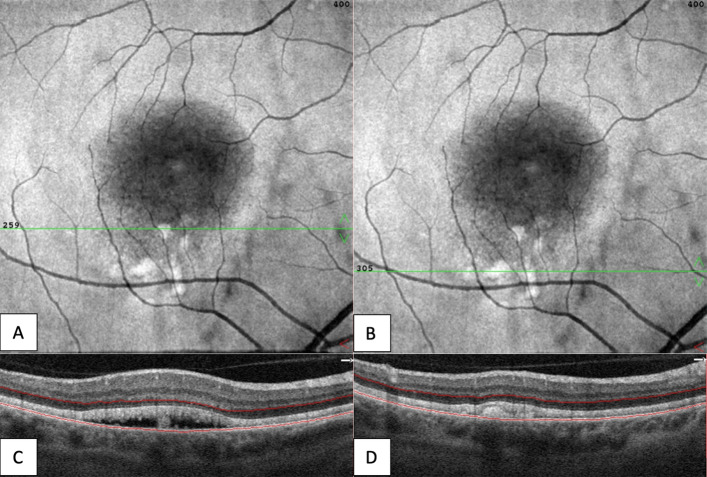
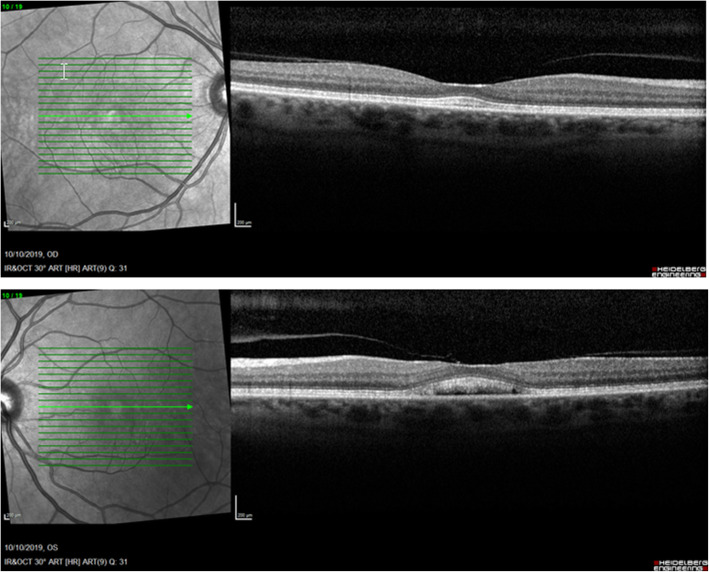
A 54-year-old woman was referred because of blurry vision in both eyes with a yellow spot in the central visual field of the left eye. These symptoms started after four treatments with pembrolizumab (a monoclonal antibody against the programmed cell death receptor-1) for a metastatic recurrent vaginal mucosal melanoma. Her best corrected visual acuity was 10/10 in both eyes with a correction of + 2.00 bilaterally. There were no inflammatory findings in the anterior segment or the vitreous. Fundoscopy revealed an attenuation of the foveal reflex with subtle yellow-white subretinal macular deposits (vitelliform lesions) in both eyes. Fluorescein angiography did not show staining or leakage in the mid-phase, neither a late staining. Spectral-domain optical coherence tomography of the macula illustrated bilateral neurosensory retinal detachment with a thick, highly reflective band at the outer photoreceptor segment. En face structural OCT at the level of the photoreceptors showed focal areas of increased signal corresponding to hyperreflective vitelliform material. The treatment with pembrolizumab was ceased immediately. During the following visits we slowly saw an improvement of the neurosensory retinal detachment. After almost four months a total resolution of the subretinal fluid was visualized in both eyes without the use of additional treatment, though the vitelliform deposits persisted.
The development of AEPVM in melanoma patients could be triggered by treatment with Pembrolizumab. Pembrolizumab has the potential to disturb indirectly the retinal pigment epithelium homeostasis with accumulation of lipofuscin deposits and subretinal fluid, both signs of AEPVM.
免疫调节疗法治疗各种癌症的应用呈上升趋势,这些免疫检查点抑制剂已知会引起眼部副作用。本文报道了一例在接受派姆单抗一线治疗期间发生的急性渗出性多形性卵黄样黄斑病变(AEPVM)。
一名 54 岁女性因双眼视力模糊,左眼中央视野有黄斑而就诊。这些症状在接受四次派姆单抗(一种针对程序性细胞死亡受体-1 的单克隆抗体)治疗转移性复发性阴道黏膜黑色素瘤后开始出现。她的最佳矫正视力在双眼均为 10/10,双眼均矫正+2.00。眼前节或玻璃体均无炎症表现。眼底检查发现双眼黄斑反射减弱,伴有细微的黄白色视网膜下黄斑沉积(卵黄样病变)。荧光素血管造影在中期无染色或渗漏,也无晚期染色。黄斑的频域光相干断层扫描显示双眼神经感觉性视网膜脱离,在外光感受器段有一条厚的、高反射带。在光感受器水平的共焦光学相干断层扫描显示,对应于高反射性卵黄样物质的焦点区域信号增强。立即停止使用派姆单抗治疗。在随后的就诊中,我们逐渐看到神经感觉性视网膜脱离有所改善。近四个月后,在未使用额外治疗的情况下,双眼均观察到视网膜下液完全消退,尽管卵黄样沉积物仍存在。
黑色素瘤患者接受派姆单抗治疗后可能会引发 AEPVM。派姆单抗有可能通过干扰视网膜色素上皮的稳态,导致脂褐素沉积和视网膜下液积聚,这两者都是 AEPVM 的特征。